The Tenth Report of Fukushima Prefecture Health Management Survey was released on February 13, 2013.
The Radiation Medical Science Center of Fukushima Medical University now has an English site where they have complete, official translation of the previous survey results.
http://www.fmu.ac.jp/radiationhealth/results/
However, the newly released result has not been officially translated yet. Excerpts of the new thyroid examination result are translated into English in this article. In addition, some critical information from the February 13, 2013 Committee meeting is included.
The thyroid examination section of the survey is shown in this link.
www.pref.fukushima.jp/imu/kenkoukanri/250213siryou2.pdf (Japanese)
It contains new thyroid examination results from April 1, 2012 through January 21, 2013, for Fiscal Year Heisei 24 (FYH24) which ends on March 31, 2013. As of January 25, 2013, 111,546 of eligible 128,082 children underwent the examination in FYH24. In FYH23, 38,114 of 47,766 eligible children underwent examination. As a whole, 149,660 of 175,848 eligible children, about half of the Fukushima children, already underwent examination.
The results compiled up to January 21, 2013 revealed that 41,947 (44.2%) of 94,975 children had thyroid ultrasound abnormalities. Together with 38,114 children (13,645 or 35.8% had thyroid ultrasound abnormalities) tested in the last half of Fiscal Year Heisei 23 (FYH23) from October 2011 through March 2012, a total of 55,592 (41.8%) of 133,089 Fukushima children have been found to have ultrasound abnormalities.
The Fukushima Prefecture Health Management Survey Planning Committee revealed that 10 of 186 eligible for the secondary examination from FYH23 were suspected of having thyroid cancer as a result of the examination. They reported that three of them were confirmed to have papillary carcinoma of thyroid gland and already had surgery. The remaining seven have 80% chance of having cancer based on their biopsy results. These children’s identities were not revealed, including their estimated thyroid exposure dose and place of residence, citing protection of their privacy.
The ten children included 3 boys and 7 girls, and their average age was 15. The average size of their tumor was 15 mm.
The three children who already had surgery include a female child between age 16 and 18 who had a C assessment in the last result, as publicized in mid-November 2012. They are all apparently doing well after surgery, being followed on an outpatient basis at this time.
There were 549 children eligible for secondary examination from FYH24, with 200 more children likely to be added from Koriyama-city and Miharu-machi where the primary examination is currently conducted. Of these 549 children, 36 have finished the secondary examination, but the results have not been released.
The percentage of abnormalities from FYH24 at 44.2% is higher than previous results of 42.7% and 43.1%, and the overall abnormality rate, for FYH23 and FYH24 combined, of 41.8% is higher than the last result of 40%. The proportion of children with nodules equal to and larger than 5.1 mm and any size cysts have increased.
******
Consideration was given to increase the number of children who could be examined by offering the examination for grade school and junior high school students at schools where the children attend . In addition, public venues with good traffic access were chosen as the examination sites.
Efforts were made to structure a more effective and efficient examination system so that the examination implementation period may be shortened:
● Try to obtain a facility where 700 to 800 may be examined per day.
● In actually implementing the examination, manage the sensitivity of the equipment in order to achieve an examination with high standards. Attempt to examine 700 to 800 children by structuring a more effective reception and guidance.
As of November 1, 2012, the thyroid examination began at facilities outside Fukushima Prefecture for those children who have evacuated Fukushima. An agreement has been reached with 77 facilities outside Fukushima Prefecture to provide examination.
*****
Note:
H23 refers to Heisei Year 23, which is the same as 2011.
FYH23 refers to Fiscal Year Heisei 23 which runs from April 1, 2011 through March 31, 2012.
H24 refers to Heisei Year 24, which is the same as 2012.
FYH24 refers to Fiscal Year Heisei 24 which runs from April 1, 2012 through March 31, 2012.
*****
For a complete English translation of the thyroid examination section of the Sixth and Seventh Reports of Fukushima Prefecture Health Management Survey, please refer to these links.
http://fukushimavoice-eng.blogspot.com/2012/07/thyroid-examination-by-fukushima.html
https://docs.google.com/file/d/0B68f83tqq7QuZUdCZXhTLVl2dEE/edit?pli=1
For a complete, official English translation of the thyroid examination section of the Eighth Report of Fukushima Prefecture Health Management Survey, please refer to this link.
www.fmu.ac.jp/radiationhealth/results/media/2_Thyroid_Ultrasound_Examination.pdf
For a complete, official translation of the thyroid examination section of the Ninth Report of Fukushima Prefecture Health Management Survey, please refer to this link.
www.fmu.ac.jp/radiationhealth/results/media/9-2_Thyroid.pdf
*****
The Tenth Report of Fukushima Prefecture Health Management Survey (excerpt)
February 13, 2013
Summary of Thyroid Examination Results ①

[Explanation of assessment classifications]
・A1 and A2 will be observed until the next round of examinations (after FYH26 or FY2014).
・B and C will undergo secondary examination. (Notice of the date and place of the secondary examination will be sent to them).
※A2 will be treated as B if the thyroid gland condition warrants the need for a secondary examination.
※Examination results for FYH24 (FY2012) include completed results up to January 21, 2013.


※Some cases have both nodules and cysts.
*********
Summary of Thyroid Examination Results ②
1. Distribution by age and gender for each assessment classification category.
(For each category the left column shows the number of boys, the middle column shows the number of girls, and the right column shows the total, based on age groups in five-year intervals.)
The upper table is for FYH23 (FY2011). The lower table is for FYH24 (FY2012), which shows the completed results up to January 21, 2013.

2. Proportion of each assessment classification category by age.
In the tables of horizontal bar graphs, the left table is for boys and the right for girls. For each age group, in five-year intervals, the top bar shows FYH23 (FY2011) and the bottom bar FYH24 (FY2012).

*********
Details of Thyroid Examination Results (FYH24 Exam: Cysts)
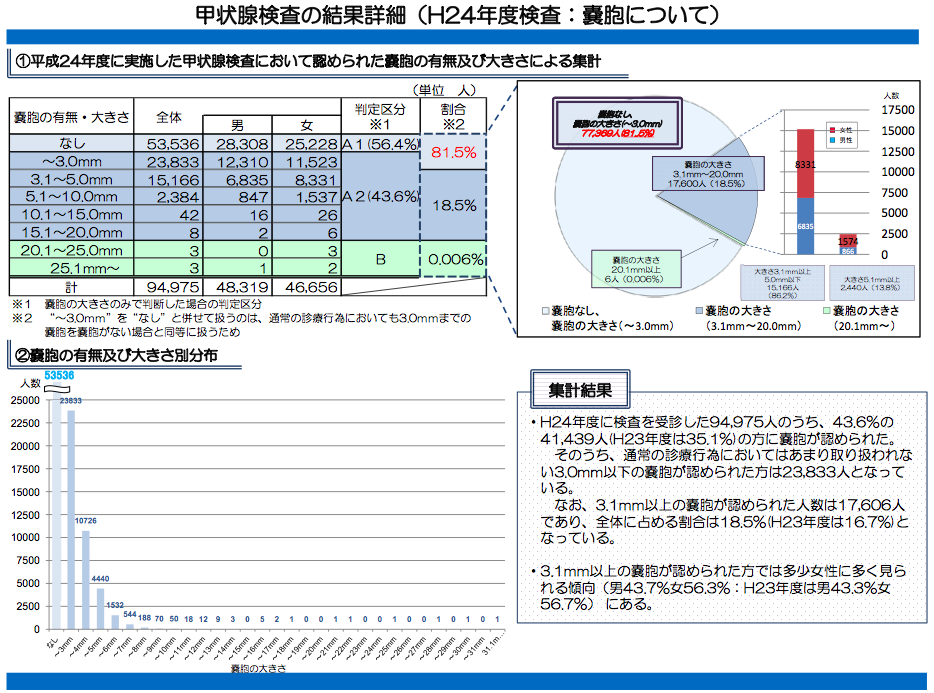
① Size breakdown of cysts found at thyroid examination conducted in FYH24 (FY2012)


Total Results
●Of 94,975 who were examined in FYH24 (FY2012), 41,439 or 43.6% (35.1% in FYH23) had cysts.
Of these, 23,833 had cysts equal to or smaller than 3.0 mm, which are considered not to be cysts in ordinary medical examinations,.
Moreover, 17,606 had cysts equal to or larger than 3.1 mm, comprising 18.5% (16.7% in FYH23) of the total examined.
● More girls tended to have cysts equal to or larger than 3.1 mm (43.7% boys and 56.3 % girls: 43.3% boys and 56.7 % girls in FYH23).
*********
Details of Thyroid Examination Results (FYH24 Exam: Nodules)

① Size breakdown of nodules found at thyroid examination conducted in FYH24 (FY2012)
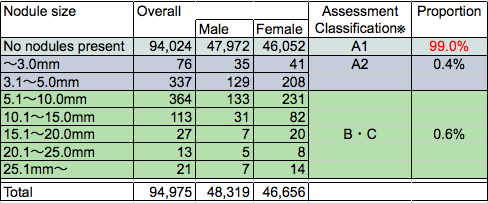
② Size distribution of nodules

Total Results
●Of 94,975 who were examined in FYH24 (FY 2012), 951 or 1.0% (1.0% in FYH23) had nodules.
●Of 951 who had nodules, 538, or 0.6% (0.5% in FYH23) of the total examined, had nodules large enough to require secondary examination.
In addition, 364 of the 538 mentioned above had nodules which were 5.1 mm to 10.0 mm in size, comprising 67.7% (68.5% in FYH23) of the 538 requiring secondary examination.
●174 had nodules which were larger than 10.0 mm, comprising 0.18% (0.15% in FYH23) of the total examined.
*********
■Summary of Secondary Thyroid Examination (All-prefecture Preliminary Examination)
FYH23 examination: 186 qualified.
151 finished and 76 had biopsy.
10 had suspicion of thyroid cancer.
3 were confirmed to have papillary thyroid cancer and had surgery.
FYH24 examination: 549 qualified with 200+ more anticipated.
Currently being conducted.
9 had biopsy, but results not released yet.
■ Implementation status of secondary thyroid examination (All-prefecture preliminary examination). (As of January 28, 2013)

※1 Those who will be re-checked at the standard examination after April 2014 due to the absence of abnormalities.
※2 Those who have moved onto regular medical care schedule, to be re-checked mostly 6 months to one year later.
■ Implementation Schedule for FYH24 and FYH 25 Secondary Thyroid Examination


The Radiation Medical Science Center of Fukushima Medical University now has an English site where they have complete, official translation of the previous survey results.
http://www.fmu.ac.jp/radiationhealth/results/
However, the newly released result has not been officially translated yet. Excerpts of the new thyroid examination result are translated into English in this article. In addition, some critical information from the February 13, 2013 Committee meeting is included.
The thyroid examination section of the survey is shown in this link.
www.pref.fukushima.jp/imu/kenkoukanri/250213siryou2.pdf (Japanese)
It contains new thyroid examination results from April 1, 2012 through January 21, 2013, for Fiscal Year Heisei 24 (FYH24) which ends on March 31, 2013. As of January 25, 2013, 111,546 of eligible 128,082 children underwent the examination in FYH24. In FYH23, 38,114 of 47,766 eligible children underwent examination. As a whole, 149,660 of 175,848 eligible children, about half of the Fukushima children, already underwent examination.
The results compiled up to January 21, 2013 revealed that 41,947 (44.2%) of 94,975 children had thyroid ultrasound abnormalities. Together with 38,114 children (13,645 or 35.8% had thyroid ultrasound abnormalities) tested in the last half of Fiscal Year Heisei 23 (FYH23) from October 2011 through March 2012, a total of 55,592 (41.8%) of 133,089 Fukushima children have been found to have ultrasound abnormalities.
The Fukushima Prefecture Health Management Survey Planning Committee revealed that 10 of 186 eligible for the secondary examination from FYH23 were suspected of having thyroid cancer as a result of the examination. They reported that three of them were confirmed to have papillary carcinoma of thyroid gland and already had surgery. The remaining seven have 80% chance of having cancer based on their biopsy results. These children’s identities were not revealed, including their estimated thyroid exposure dose and place of residence, citing protection of their privacy.
The ten children included 3 boys and 7 girls, and their average age was 15. The average size of their tumor was 15 mm.
The three children who already had surgery include a female child between age 16 and 18 who had a C assessment in the last result, as publicized in mid-November 2012. They are all apparently doing well after surgery, being followed on an outpatient basis at this time.
There were 549 children eligible for secondary examination from FYH24, with 200 more children likely to be added from Koriyama-city and Miharu-machi where the primary examination is currently conducted. Of these 549 children, 36 have finished the secondary examination, but the results have not been released.
The percentage of abnormalities from FYH24 at 44.2% is higher than previous results of 42.7% and 43.1%, and the overall abnormality rate, for FYH23 and FYH24 combined, of 41.8% is higher than the last result of 40%. The proportion of children with nodules equal to and larger than 5.1 mm and any size cysts have increased.
******
Consideration was given to increase the number of children who could be examined by offering the examination for grade school and junior high school students at schools where the children attend . In addition, public venues with good traffic access were chosen as the examination sites.
Efforts were made to structure a more effective and efficient examination system so that the examination implementation period may be shortened:
● Try to obtain a facility where 700 to 800 may be examined per day.
● In actually implementing the examination, manage the sensitivity of the equipment in order to achieve an examination with high standards. Attempt to examine 700 to 800 children by structuring a more effective reception and guidance.
As of November 1, 2012, the thyroid examination began at facilities outside Fukushima Prefecture for those children who have evacuated Fukushima. An agreement has been reached with 77 facilities outside Fukushima Prefecture to provide examination.
*****
Note:
H23 refers to Heisei Year 23, which is the same as 2011.
FYH23 refers to Fiscal Year Heisei 23 which runs from April 1, 2011 through March 31, 2012.
H24 refers to Heisei Year 24, which is the same as 2012.
FYH24 refers to Fiscal Year Heisei 24 which runs from April 1, 2012 through March 31, 2012.
*****
For a complete English translation of the thyroid examination section of the Sixth and Seventh Reports of Fukushima Prefecture Health Management Survey, please refer to these links.
http://fukushimavoice-eng.blogspot.com/2012/07/thyroid-examination-by-fukushima.html
https://docs.google.com/file/d/0B68f83tqq7QuZUdCZXhTLVl2dEE/edit?pli=1
For a complete, official English translation of the thyroid examination section of the Eighth Report of Fukushima Prefecture Health Management Survey, please refer to this link.
www.fmu.ac.jp/radiationhealth/results/media/2_Thyroid_Ultrasound_Examination.pdf
For a complete, official translation of the thyroid examination section of the Ninth Report of Fukushima Prefecture Health Management Survey, please refer to this link.
www.fmu.ac.jp/radiationhealth/results/media/9-2_Thyroid.pdf
*****
The Tenth Report of Fukushima Prefecture Health Management Survey (excerpt)
February 13, 2013
Summary of Thyroid Examination Results ①
[Explanation of assessment classifications]
・A1 and A2 will be observed until the next round of examinations (after FYH26 or FY2014).
・B and C will undergo secondary examination. (Notice of the date and place of the secondary examination will be sent to them).
※A2 will be treated as B if the thyroid gland condition warrants the need for a secondary examination.
※Examination results for FYH24 (FY2012) include completed results up to January 21, 2013.
※Some cases have both nodules and cysts.
*********
Summary of Thyroid Examination Results ②
1. Distribution by age and gender for each assessment classification category.
(For each category the left column shows the number of boys, the middle column shows the number of girls, and the right column shows the total, based on age groups in five-year intervals.)
The upper table is for FYH23 (FY2011). The lower table is for FYH24 (FY2012), which shows the completed results up to January 21, 2013.
2. Proportion of each assessment classification category by age.
In the tables of horizontal bar graphs, the left table is for boys and the right for girls. For each age group, in five-year intervals, the top bar shows FYH23 (FY2011) and the bottom bar FYH24 (FY2012).
*********
Details of Thyroid Examination Results (FYH24 Exam: Cysts)
① Size breakdown of cysts found at thyroid examination conducted in FYH24 (FY2012)
Total Results
●Of 94,975 who were examined in FYH24 (FY2012), 41,439 or 43.6% (35.1% in FYH23) had cysts.
Of these, 23,833 had cysts equal to or smaller than 3.0 mm, which are considered not to be cysts in ordinary medical examinations,.
Moreover, 17,606 had cysts equal to or larger than 3.1 mm, comprising 18.5% (16.7% in FYH23) of the total examined.
● More girls tended to have cysts equal to or larger than 3.1 mm (43.7% boys and 56.3 % girls: 43.3% boys and 56.7 % girls in FYH23).
*********
Details of Thyroid Examination Results (FYH24 Exam: Nodules)
① Size breakdown of nodules found at thyroid examination conducted in FYH24 (FY2012)
② Size distribution of nodules
Total Results
●Of 94,975 who were examined in FYH24 (FY 2012), 951 or 1.0% (1.0% in FYH23) had nodules.
●Of 951 who had nodules, 538, or 0.6% (0.5% in FYH23) of the total examined, had nodules large enough to require secondary examination.
In addition, 364 of the 538 mentioned above had nodules which were 5.1 mm to 10.0 mm in size, comprising 67.7% (68.5% in FYH23) of the 538 requiring secondary examination.
●174 had nodules which were larger than 10.0 mm, comprising 0.18% (0.15% in FYH23) of the total examined.
*********
Implementation Status of FYH24 (FY2012) Secondary Thyroid Examination
■Summary of Secondary Thyroid Examination (All-prefecture Preliminary Examination)
FYH23 examination: 186 qualified.
151 finished and 76 had biopsy.
10 had suspicion of thyroid cancer.
3 were confirmed to have papillary thyroid cancer and had surgery.
FYH24 examination: 549 qualified with 200+ more anticipated.
Currently being conducted.
9 had biopsy, but results not released yet.
■ Implementation status of secondary thyroid examination (All-prefecture preliminary examination). (As of January 28, 2013)
※1 Those who will be re-checked at the standard examination after April 2014 due to the absence of abnormalities.
※2 Those who have moved onto regular medical care schedule, to be re-checked mostly 6 months to one year later.
■ Implementation Schedule for FYH24 and FYH 25 Secondary Thyroid Examination
Implementation Schedule for FYH25 Thyroid Examination
(All-prefecture Preliminary Examination)