Shunichi Yamashita was in the United States on March 11, 2013, giving a keynote address at the 2013 Annual Meeting of the National Council on Radiation Protection and Measurements. http://www.ncrponline.org/
The video of the address was transcribed, word for word as much as possible, so that it might be translated into Japanese.
The original English transcript is published below for those interested in knowing what Yamashita said. The image of each slide is followed by what he said about it.
*****
10th Annual Warren K. Sinclair Keynote Address: Fukushima Nuclear Power Plant Accident and Comprehensive Health Risk Management
Shunichi Yamashita, M.D., Ph.D.
Video for Yamashita’s lecture at the March 11 NCRP annual meeting:
PowerPoint slides:
*****
Slide 2
The recording apparently began in the middle of Slide 2.
Slide 2: (….) many countries and international organizations, just after Great East Japan Earthquakes, especially from the United State, Operation Tomodachi, worked very well for the Japanese.
Slide 3

Slide 3: Today I would like to present the Fukushima nuclear power plant accident and the comprehensive health risk management. Because as John introduce my career, I originally from Nagasaki, you know, Hiroshima/Nagasaki. We were working for a long time to help the survivors. I am also deeply committed to Chernobyl project since 1991.
Just after the Fukushima accident, I have been dispatched from Nagasaki University to Fukushima to assist not only emergency radiation medicine but established for the residents’ health care and also the health management. Therefore, today’s my talk is merely to focusing on Chernobyl issues and Fukushima’s health management survey problem.
Slide 4
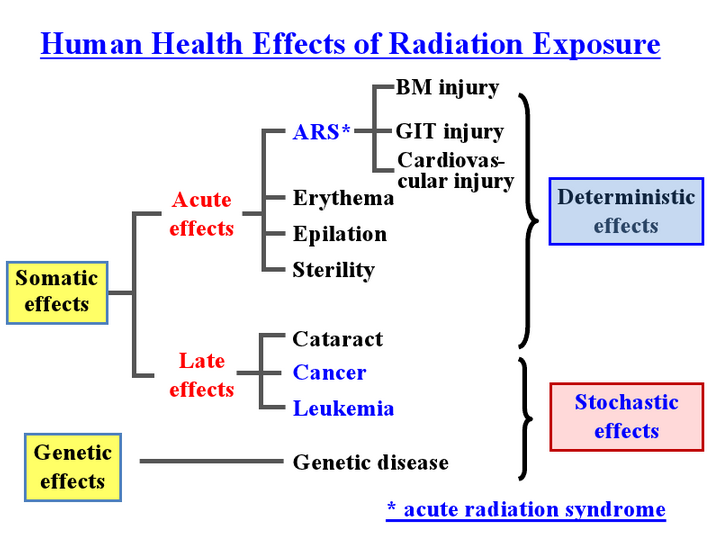
Slide 4: As all of you know, the health effect are simply categorized by acute effects and late effect. It depend on the dose. We know the importance of dose. How much dose received? But in general speaking, people they don’t know. For example, nuclear reactors accident don’t equal A-bomb survivors datas such as acute radiations at all. This may confuse in the current situation in Fukushima. So we need carefully think about differentiate the deterministic effect, it’s a kind of the large amount of radiation exposure. But today I will talk about mainly low-dose radiation effect, so-called stochastic effect.
Slide 5
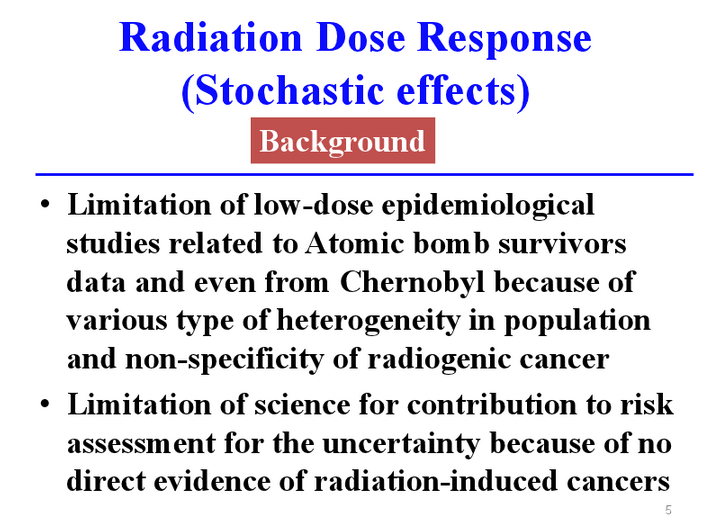
Slide 5: However, it’s very difficult to explain to the public what is the stochastic effect. Even a long time, RERF, Radiation Effect Research Foundation Hiroshima/Nagasaki, was working very hard for A-bomb survivors’ data, and also we working a long time in Chernobyl, but this is limitation of low-dose epidemiological studies exist. It means limitation of science to contribution to risk assessment for the uncertainty exists because of no direct evidence of radiation-induced cancer.
Slide 6
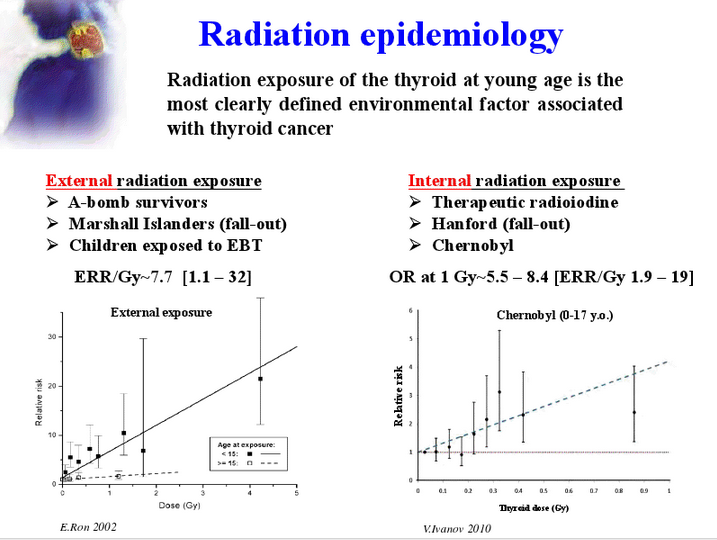
Slide 6: However, we already know very good data by radiation epidemiologies. Especially today I would like to concentrate on the thyroid carcinogenesis. Exposure of radiation on thyroid of young age is a most clearly defined environmental factor associated with thyroid cancer, either by external or internal radiation exposure, on the basis of large cohort study of A-bomb survivors and also in Chernobyl. These two slides show dose-response relationship between thyroid dose and relative risk of thyroid cancer, either external or internal. Very similar tendency because there is a unit of the Sievert, means equal or equivalent biological effect either external or internal. So we know more than 100 mSv can cause increase of thyroid cancer in dose-responsive manner.
Slide 7
Slide 7: About half of my presentation I would like to concentrate what really we learned from Chernobyl and how to apply lesson learned from Chernobyl to Fukushima. Very sadly, at the time of Chernobyl accident in 1986, it was a Cold War age. The world was divided east and west. This is really man-made disaster. And very unfortunately public protection against short-lived radioactive iodines and greater internal exposure subsequently occurred by radioactive cesium. Both were through food chain and drink, were not inhibited or controlled very well. And then eventually, December 1991 former Soviet Union has collapsed. The people suffered a lot from the Chernobyl. Impact of psychosocial and mental consequences were so huge when we worked at the time 1991, so there were confusion and the myth inside of Chernobyl. We learned a lot of things.
Slide 8
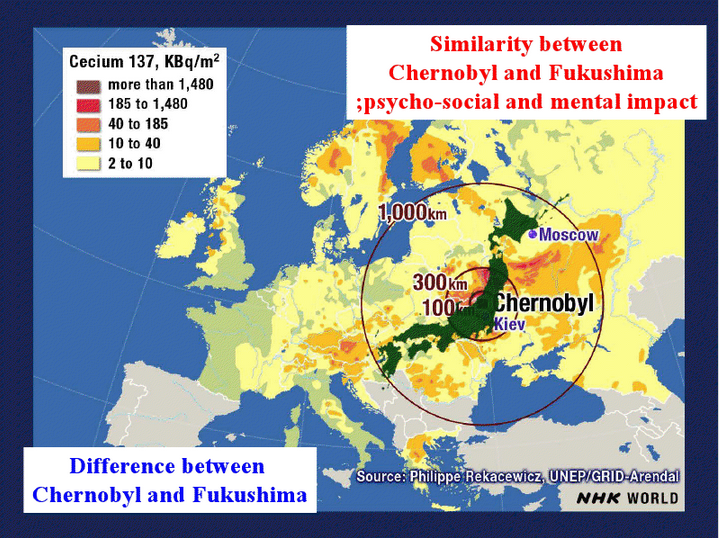
Slide 8: As all of you know, this is a map of radioactive cesium 137 contaminated entire European region, compared to the Japan, Japanese map. Just after the Fukushima accident, people were worried too much Fukushima may become similar to Chernobyl. But that’s not right. Of course, there is a big difference between Chernobyl and Fukushima. However, very much similarity also exists between Chernobyl and Fukushima, so-called psychosocial and mental impact. Very sadly we are now in the middle of this kind of the confusion in Fukushima.
Slide 9
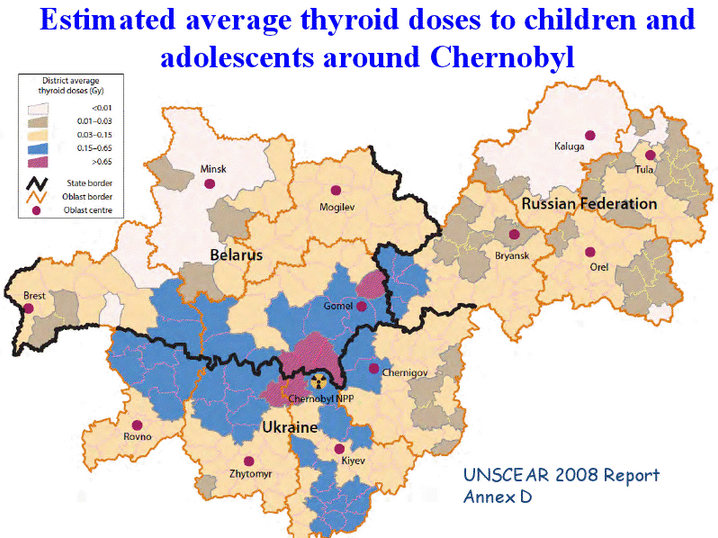
Slide 9: This map shown on the estimated average thyroid dose to children and adolescents around Chernobyl reported by UNSCEAR 2008. Chernobyl accident occurred 1986 this kind of the slide available more than 20 years later, because radioactive iodine to the thyroid was very much difficult to be examined and evaluated. According to this map, average dose of children who suffered in these area was around 500 mSv. At those exposures very, very important to consider the late effect of radiation.
Slide 10
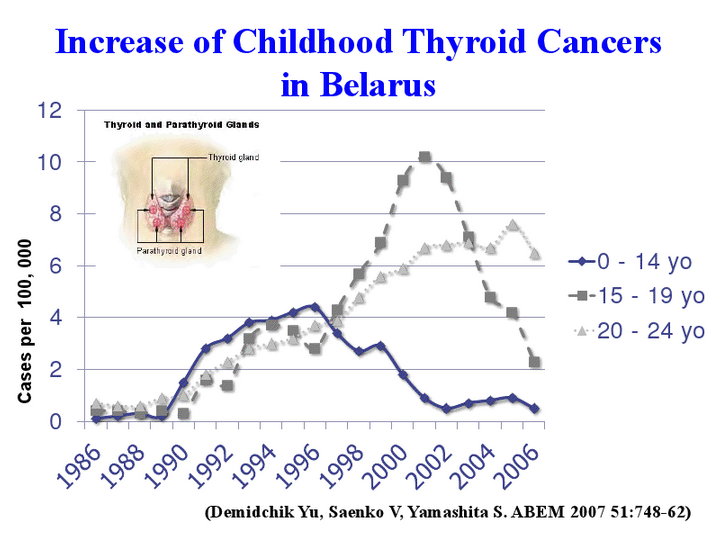
Slide 10: According to such kinds of the data available later, and we also encountered in 1990, 1992, rapid increase of childhood thyroid cancer. This is depict mainly the Belarussian data, age less than 14 years old, 15-19, 20-24. Then on the year by year, the peak of the childhood thyroid cancer shifted from infant, adolescent, and young adult. Because the target of children who developed thyroid cancer by age less than 10 years old. Especially the age less than five. Because later we realized our children drank contaminated milk just after Chernobyl accident.
Slide 11
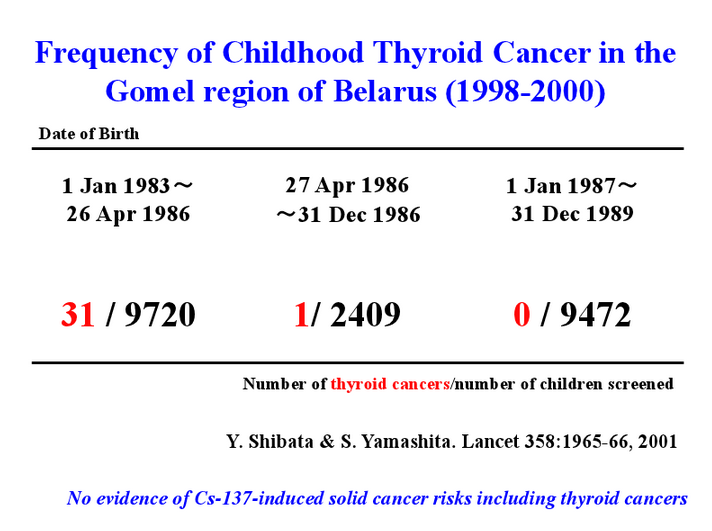
Slide 11: However, as I said in the previous slide for the UNSCEAR data, it is almost impossible to evaluate real thyroid dose by radioactive iodine. Because of the half life of 8 days, it immediately disappeared. When we entered Chernobyl in 1991, no radioactive iodine exist. So therefore we compared the children’s incidence of thyroid cancer between age at the time of 0 to 3 years old and age after that they born just after the accident. Very interestingly, the children who were born at the time of the accident, 0 to 3 years old, is highly prevalent of thyroid cancer. But after accident one years laters, no increase of thyroid cancer observed. So this is another direct evidence, but indirect evidence of thyroid cancer may caused by radioactive iodine. Fortunately, they are still living at the contamination of radioactive situations, but no increase of other significant cancers in those children. However, in Fukushima, the people worried too much of radioactive iodine and also radioactive cesium may cause any kind of the cancer. We deny such kind of data based on the Chernobyl, however, the public perception so-called misunderstanding prevailed entire Japan.
Slide 12
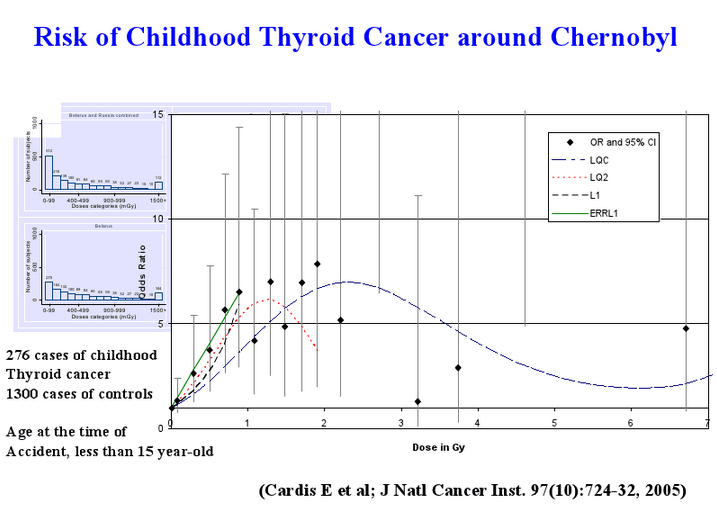
Slide 12: According to other joint project on the case control studies, it's also clearly shown the increase of thyroid cancer by in dose-responsibly by radioactive iodine. These data also reconfirmed by United States and Belarus and United States-Ukranian cohort project recently. This is really important to understand the dose-responsiveness of how much they received thyroid dosing.
Slide 13
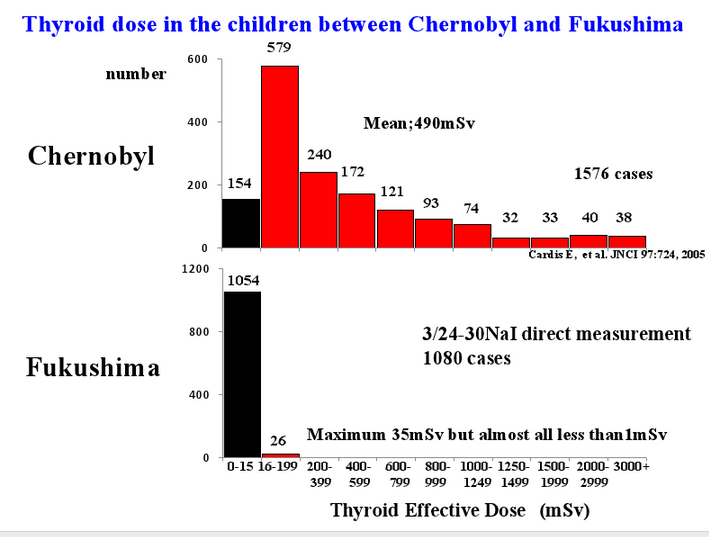
Slide 13: Compared to the Chernobyl datas and in upper panels, I mentioned averaged in doses of about 500 mSv thyroid dose. In Japan, fortunately, just after the accident, March 24th to 30, 180 children were measured directly by NaI counters, and almost all were less than 1 mSv. So this is very good news. However, this is too small number of the childrens. We need carefully to follow those who were evacuated from the Fukushima area.
Slide 14

Slide 14: And also another important factor is iodine concentration in the thyroid. Fukushima and Chernobyl is completely different. In land of Chernobyl are chronically iodine deficient areas and then received radioactive iodine. However, Fukushima is already saturated, compared to the Fukushima, such kind of thyroid iodine dose. So iodine also another important factor. Unfortunately in Japan, such kind of the iodine thyroid-blocking was not effectively administrated by the Japanese government. However, the doses are so small. So we don’t need to worry too much about radioactive iodine to the thyroid gland.
Slide 15
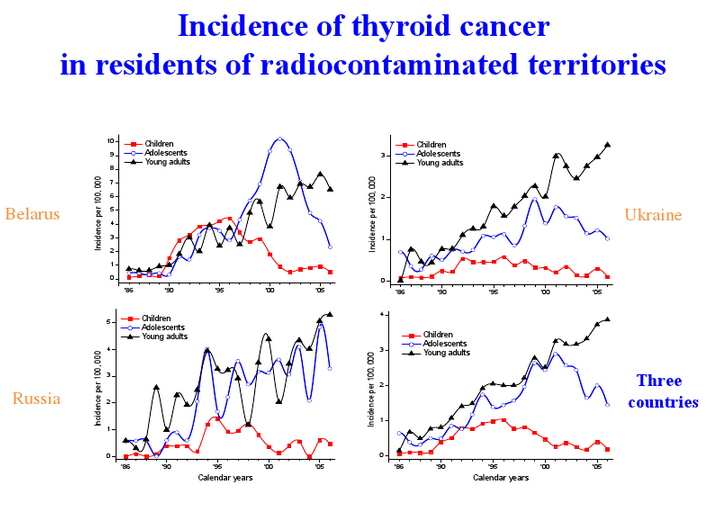
Slide 15: According to the three countries including Belarus, Ukraine and Russia, same tendency of increase of child thyroid cancer are reported. The different age group, children, adolescent and young adult. Three countries summarized also showed now the peak of the thyroid cancers were shifted from children, to adolescent and finally recently to the adult. Even one-time exposure just after the Chernobyl accident, the risk has continued especially for the younger children. We need to clarify the mechanisms of biological effects of this kind of the radiation-induced thyroid cancers.
Slide 16
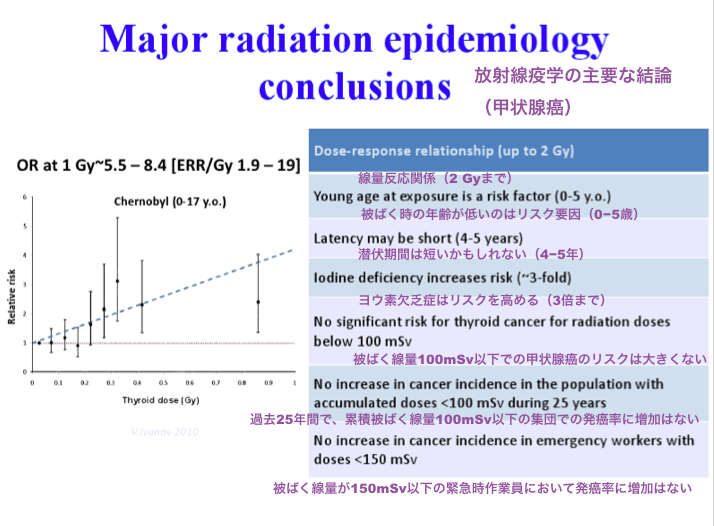
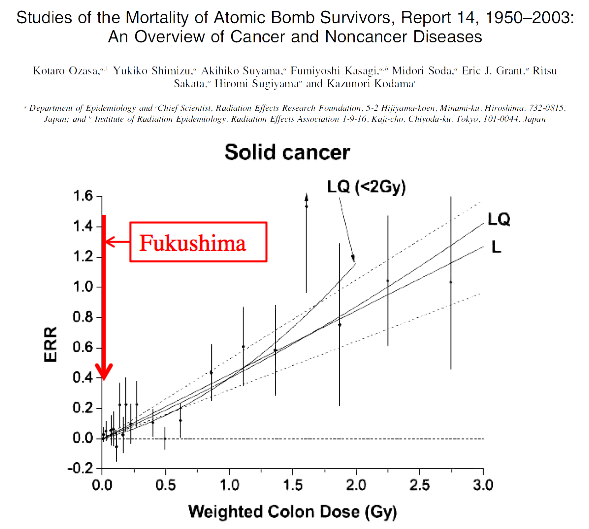
Slide 16: In conclusion of the good radiation epidemiological studies indicated the several important point, especially dose-response relationship between 100 mSv up to 2,000 mSv. Especially younger age is at the exposure is a risk factors. Latency occur, probably from 4 to 5 years even in childrens. Iodine deficiency increases the risks. And below 100 mSv it’s very hard to detect any increase of thyroid cancer. No increase in cancer incidence in population with less than based on 100 mSv the past 25 years. Besides this kind of the Chernobyl children’s datas, emergency workers data suggest less than 150 mSv, there are no increase in cancer incidence. This is exactly we learn from Chernobyl. However, Fukushima, very difficult even we are using this kind of the evidence, a fact, but people cannot accept this kind of the data.
Slide 17
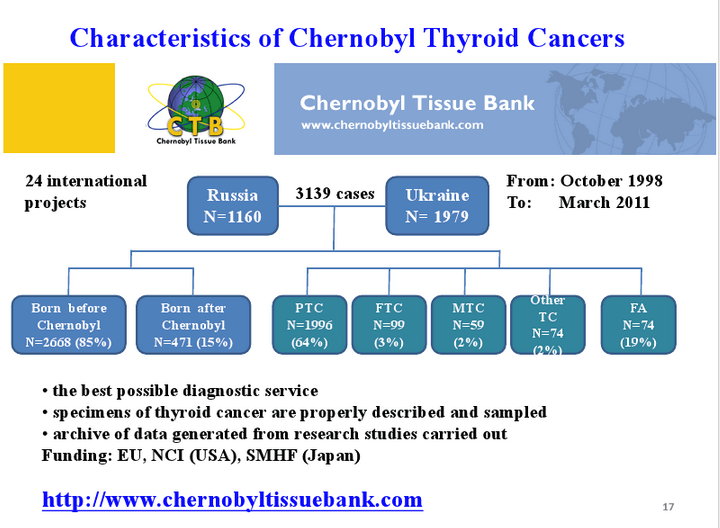
Slide 17: On the basis of the Chernobyl Thyroid Tissue Banks, we also categorizing what is the direct signature or relationship between radiation exposure and thyroid carcinogenesis. 1998 to 1999 we have established that kind of the Chernobyl Tissue Bank together with Russia, when originally Belarussian involved, but now it flopped. So now we have collected more than 3,000 cases of thyroid diseases in this tissue banks. Using this tissue bank, we are now analyzing pathological and clinical characteristic of Chernobyl papillary thyroid cancers in comparison with spontaneous thyroid cancer.
Slide 18
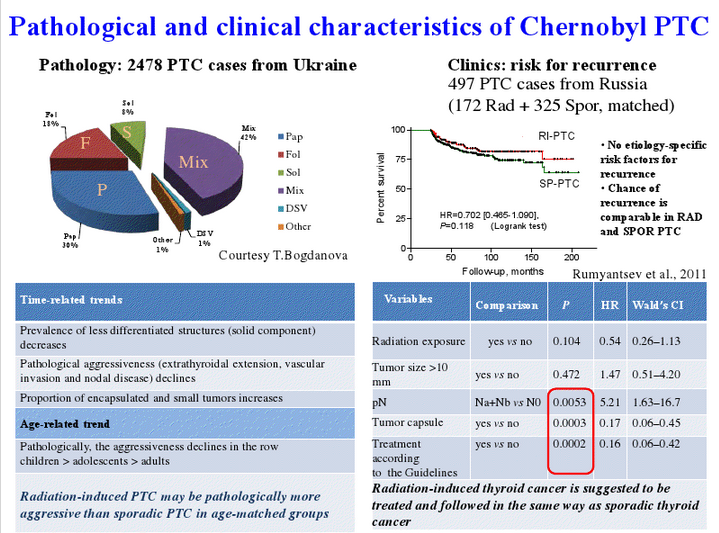
Slide 18: Very much difference exists on the pathological finding of Chernobyl-related papillary thyroid cancer as it’s closely related age dependences. Young children has very unique papillary thyroid cancers histologically in comparison with other papillary thyroid cancers. We learned a lot of things: time-related trends of childhood thyroid cancers and age-related trend of thyroid cancer. However, a risk of thyroid cancer such as recurrences are a lot different between two groups, spontaneous-occurring and radiation-induced thyroid cancer. This kind of the hint also gave us a very important position when we started Fukushima health medical survey programs including thyroid ultrasound examination in children in Fukushima.
Slide 19
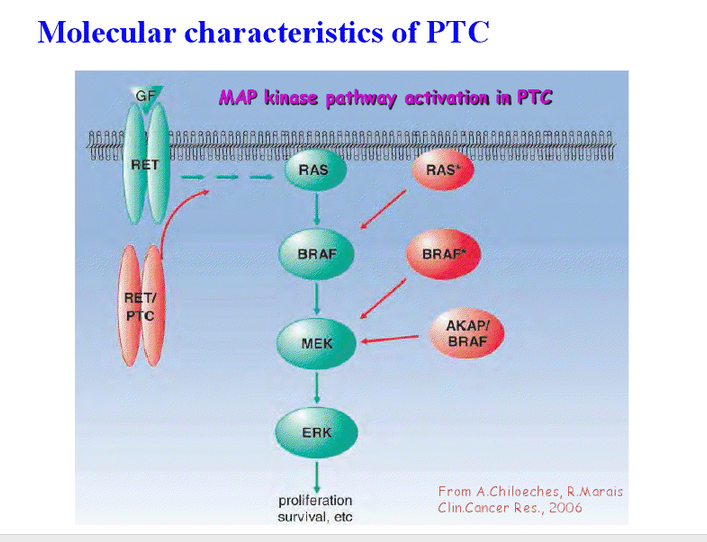
Slide 19: As you may know, the mechanism of thyroid cancer now clearly characterized using the different genetic abnormality. Mainly papillary thyroid cancer occur in the pathway somewhere from RET-RAS-BRAF-MEK-ERK MAP kinase activities are over-activated by somewhere the point of mutation or rearrangement. This is very unique case to learn the mechanisms of papillary thyroid cancer carcinogenesis.
Slide 20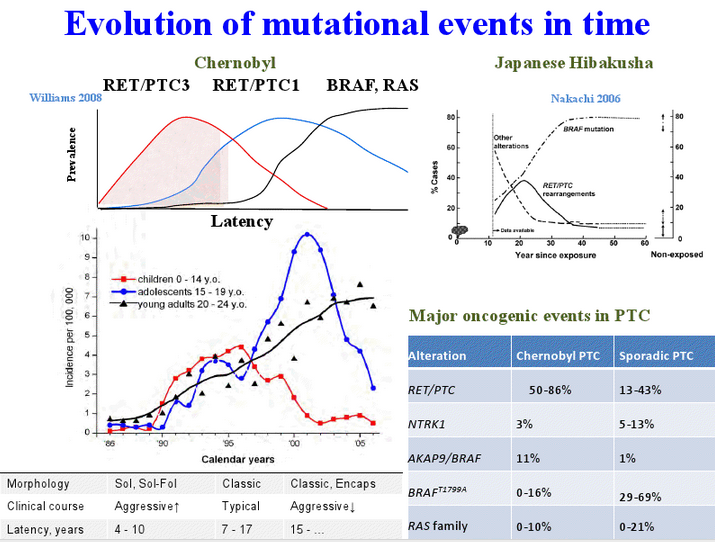
Slide 20: We also clearly find, through the mutational events, the time different, from the Chernobyl, what kind of the genetic abnormality exists in Chernobyl. I show in the left panel the latency is very clearly occurred. Difference of characteristic of the Chernobyl thyroid gene abnormality, such as the first younger children’s and shorter latencies predominantly express rearrangement of RET/PTC3 and RET/PTC1. This is a gene arrangement and just by DNA double-strand breaks. However longer latencies and also older age showed a high frequency of BRAF point mutation. Even the same type of papillary thyroid cancer, genetic background are completely different between two groups, children and adults papillary thyroid cancer. Similar tendency also opens up in Japanese A-bomb survivors, reported by RERF. So this is also very important to seek for the mechanisms of radiation-induced carcinogenesis.
Slide 21
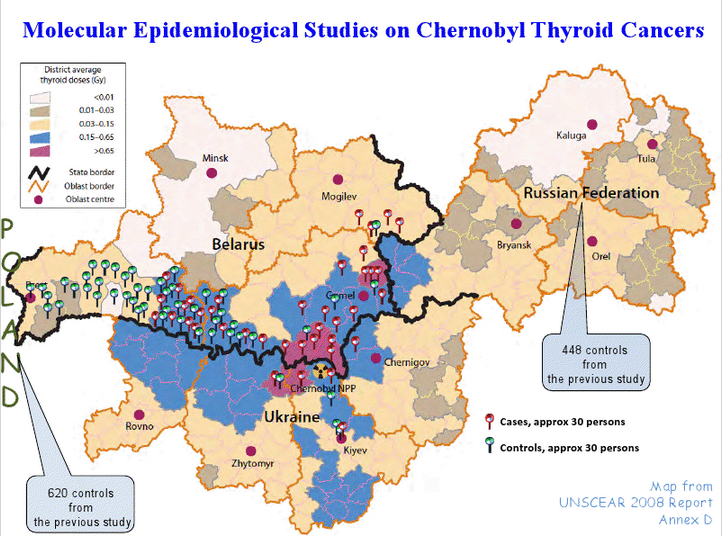
Slide 21: However, the same radiation exposed for those children, only a small part of those children occur thyroid cancer. Majority of the children never occur thyroid cancer. So we have focused on two qualifying molecular epidemiological studies on thyroid cancer are shown in this slide. We collected nearly 1,000 childhood thyroid cancer samples, it’s a blood, with each bar indicates approximately 30 persons exists in these areas, Belarus, Ukraine and Russian Federation, together with controls in same areas. We collected more than 1,000 cases and more than 1,000 control cases.
Slide 22
Slide 22: And then GWAs indicated very clear tendencies of cancer-susceptibility genes, and this FOXE1 chromosome 9. This is FOXE1, a thyroid-specific transcription factor 2. And also we confirmed other related genes. Interestingly, those genetic background SNPs abnormalities highly expressed in Chernobyl thyroid cancer.
Slide 23
Slide 23: Our final analysis is clearly indicates a big difference between cases and controls, control now nearly 2,000 cases.
Slide 24
Slide 24: We have reported already 2010 this type of the FOXE1 is a major genetic determinant for radiation-related thyroid cancer in Chernobyl. Of course, those children who develop thyroid cancer carried not only radiation-specific SNP types but also sporadic SNP types were overlapped in two groups. Not only radiation but also genetic susceptibility of thyroid carcinogenesis based on the common genetic background are very important in addition to environmental factor such as radiation.
Slide 25 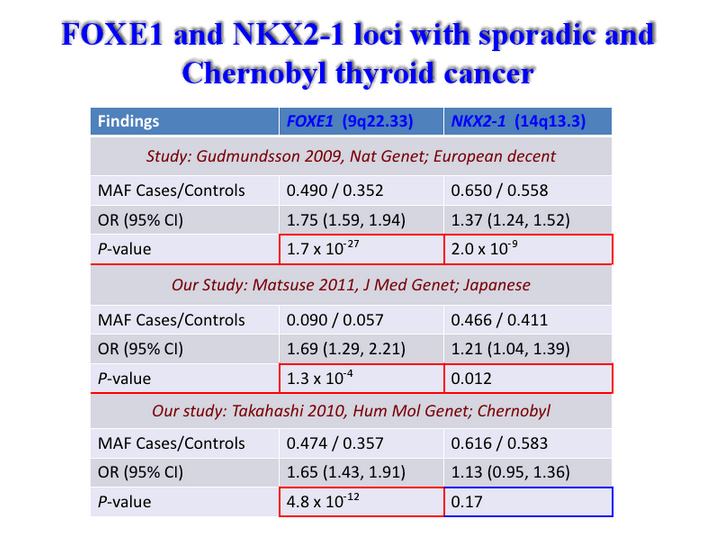
Slide 25: So we now then concentrated on the other population, not only European people but also Japanese people. Similar tendencies of this SNPs abnormality exist thyroid carcinogenesis FOXE1. So now we know, realize the FOXE1 is one of the candidate gene for thyroid carcinogenesis. This is also very unique finding to follow extensively to the Fukushima area.
Slide 26
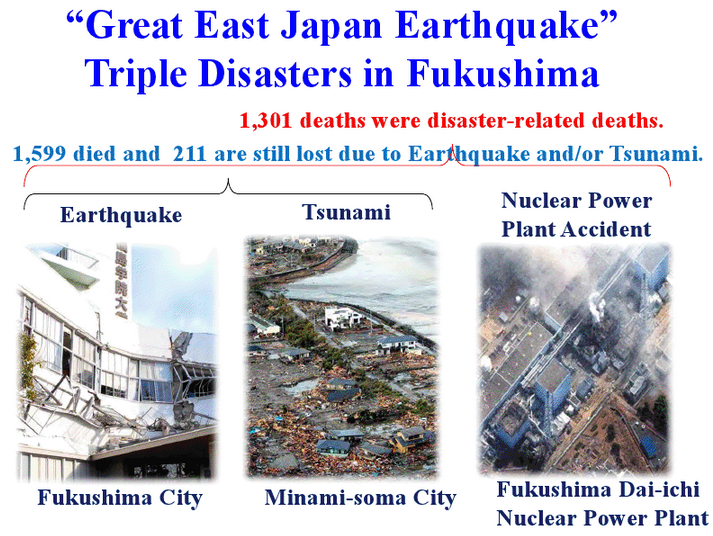
Slide 26: Now the second part of my presentation I would like to concentrate on Great East Japan Earthquakes. Just two years ago it happened. Earthquake, tsunami, and nuclear power plant accident. It’s really multidimensional disaster in Fukushima. In Fukushima, among 20,000 were killed by the Great East Japan Earthquake, 1,600 died and 202 missing in Fukushima. In addition, more than 1,000 dead were disaster-related deaths. It means during evacuation time or after evacuated time. Even though there were no acute radiation injury, there were deaths due to evacuation. It’s really sad situation. And how to prepare for the medical response are also very important to think about this kind of the disaster-related death.
Slide 27
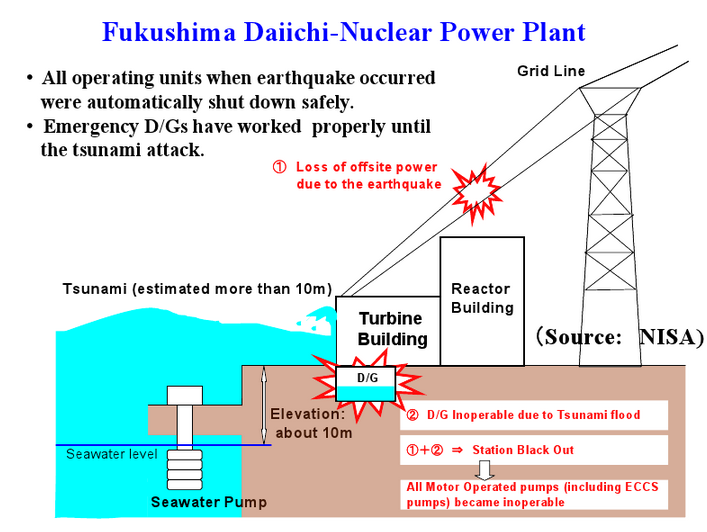
Slide 27: As all you know, Fukushima Dai-ichi nuclear power plant has completely lost the electricity by tsunami. Fortunately, after earthquake everything had stopped. So we failed to continuous cooling without any electricity back-up.
Slide 28
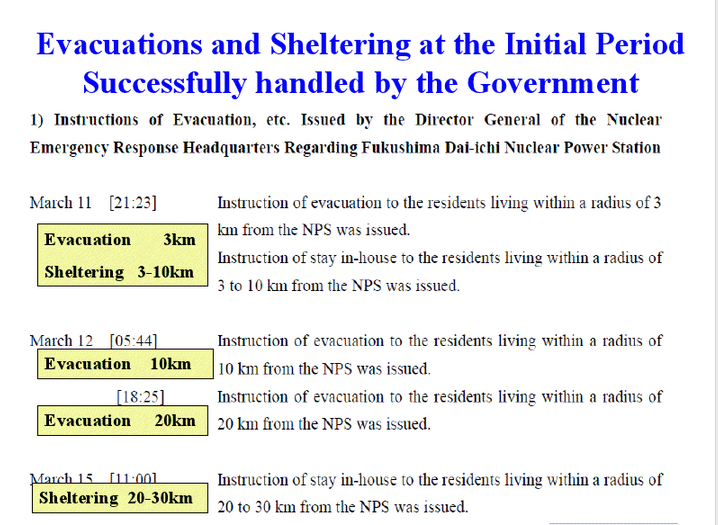
Slide 28: Japanese government ordered immediately evacuation and sheltering. According to this slide, March 11, March 12, March 15, going to 3km, then 10km, from 10km to 20km even after they wanted and the value is 20 km. Between 20-30 km were indoor, house evacuated were recommended on March 15. Then we received massive fallout from the Fukushima Dai-ichi nuclear power plant.
Slide 29
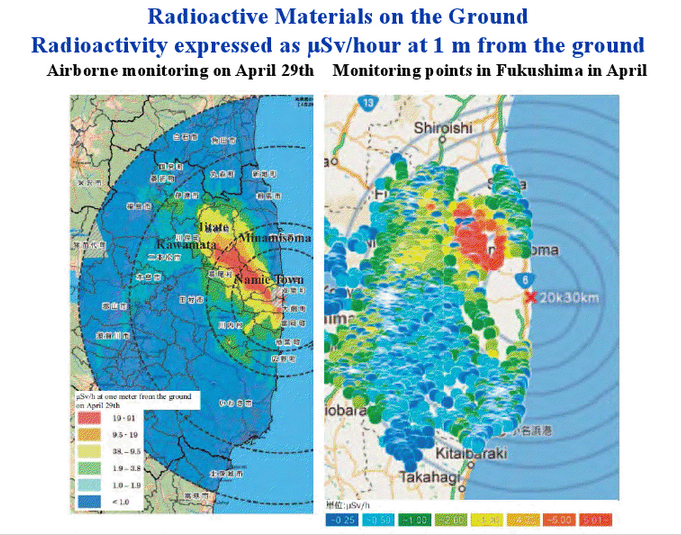
Slide 29: And then eventually the areas are contaminated as shown in this slide. Airborne monitoring April 29th, and also monitoring points were shown in this slide μSv. Red one showed more than 19 μSv/h, blue one less than 1 μSv/h. This situation is not continuing. And two years later the accident, very fortunately, almost half levels of each, because of the radioactive cesium 134 very slowly influenced in the half-life of 2 years. So therefore almost half level from the beginning airborne monitoring data are decreased in Fukushima.
Slide 30
Slide 30: This nuclear reactor accident is not horrific disaster. It’s exactly industrial crisis and environmental damages. And government ordered evacuation and sheltering, it worked sufficiently. Therefore the dose exposed for the population are dramatically decreased after evacuations. However, there are many problems exist such as nuclear worker, operational staff, and emergency response personnel also exposed to certain levels of radiation. Since there are much concern about the levels of exposure and effects both on general public and workers, we are prepared to collect and offer further information to the world.
Slide 30
Slide 31: Public concern is major issues. They worry about long-term health effect of radioactive contamination. Especially they are sparking anger, anxiety and distrust toward the government handling, even we experts are targeted from the public and the mass media. Bans of food shipments from contaminated areas, too much anxiety about food safety are ruining farmers’ livelihoods and raise another concerns about their ability to resume their livelihoods. The role of experts and academic societies are important but reliabilities and credibility both were lost by confusion and misunderstanding partly due to an inappropriate and immature media literacy.
Slide 32
Slide 32: I was dispatched March 18, one weeks after the accident here in Fukushima Medical University. They worked very hard to support the evacuees. But, the bed is about 800, the staff is more than 100-1,500, They were very much concerned and afraid, almost they are also escaping from this university, 60 km distance from the Fukushima Dai-ichi.
Slide 33
Slide 34
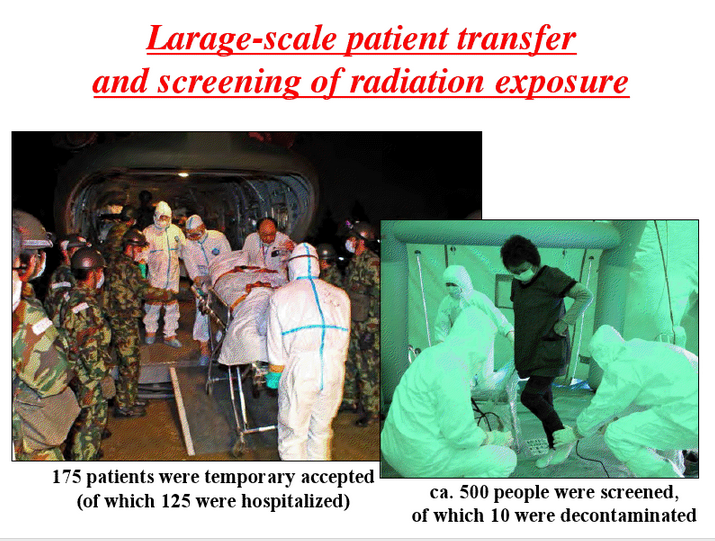
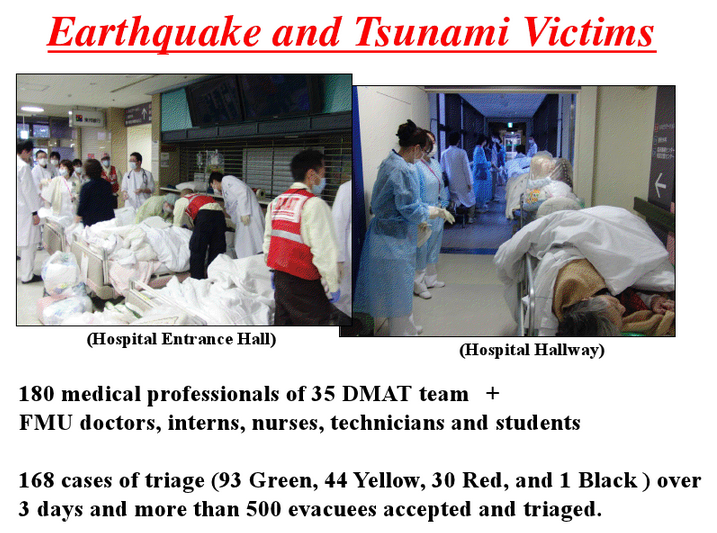
Slides 33-34: So we worked together with them to respond to earthquake and tsunami victims and also large-scale patient transfer and also screen the people who were received radiation fallout. There were many rooms for improvement, however, the medical staff even Self-Defense or the firemen and policemen worked very, very much hard from the beginning.
Slide 35
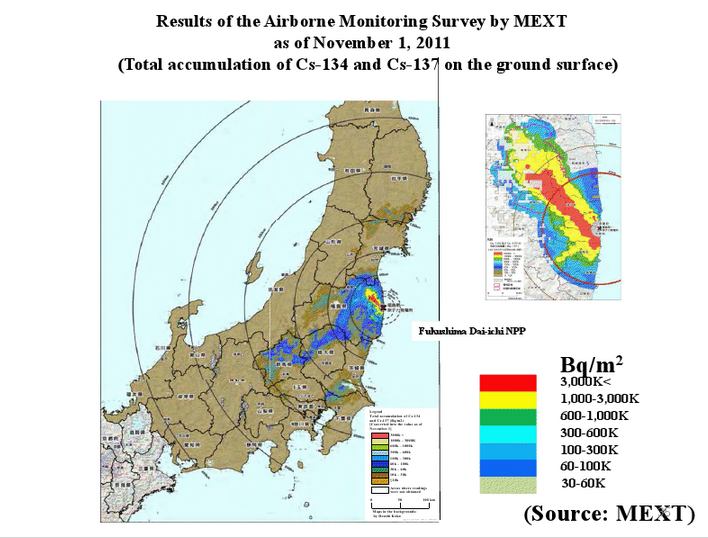
Slide 35: And finally, this kind of the map are shown entire Japan, mainly focusing on Fukushima and the neighboring prefecture.
Slide 36
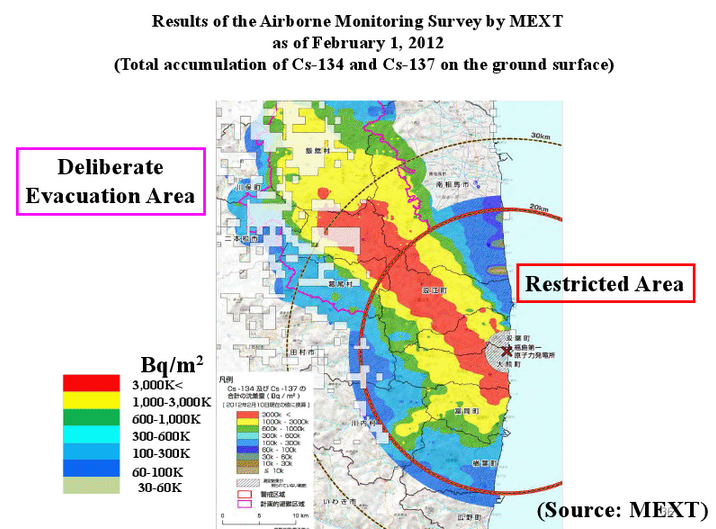
Slide 36: Now the targeted area around 30 km zone. Within 20 km we call “Restricted Area.” But even the west and north areas from the Namie to Iitate-mura we call “Deliberate Evacuation Areas.” Also the people evacuated from these contaminated areas.
Slide 37
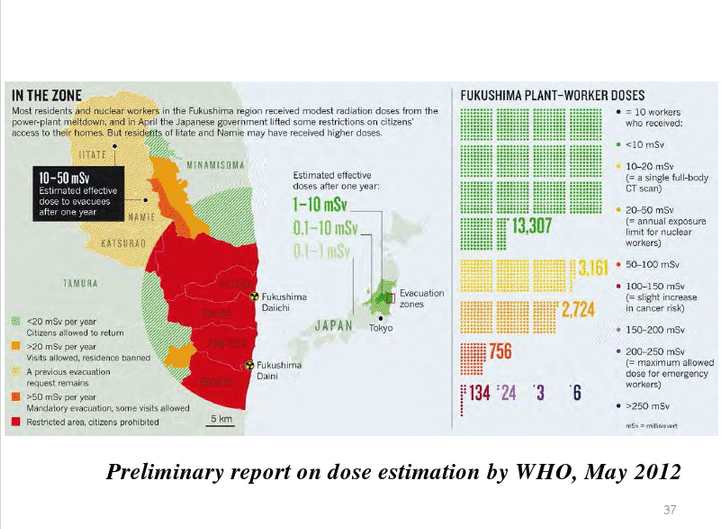
Slide 37: According to the preliminary data by WHO, their estimated last May, how much they received in population in Fukushima. This is very conservative and theoretical data from people who were continuously residing first four months and then eating contaminated food. It’s very much theoretical, not far beyond the reality to the public. And this is very important to consider how much they received the dose. Simultaneously Fukushima plant workers also measured in this type of the studies. More than 200 mSv received workers exists. This is really important target for long-term health monitoring especially needed for those people.
Slide 38
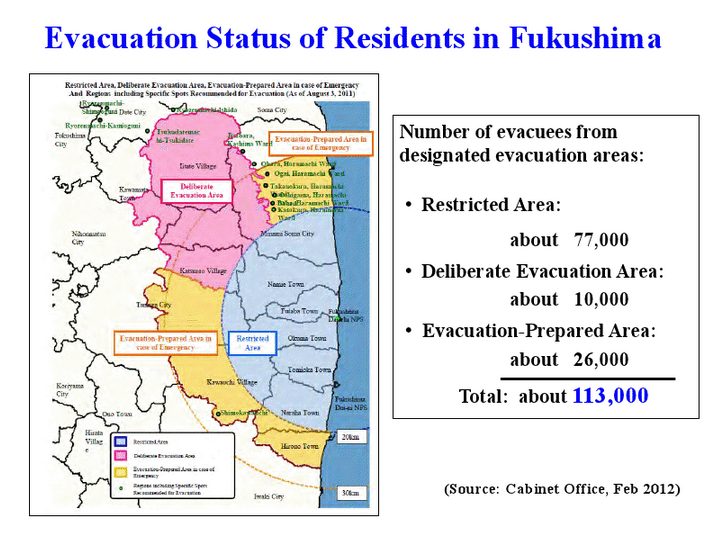
Slide 38: Now in Fukushima are categorized these areas. Restricted Area about 77,000 evacuate. Deliberate Evacuation Area is about 10,000. Evacuation Prepared Area, 26,000. A total about 113 are evacuated in these areas. Besides these areas, within 30 km, total 210,000 are evacuated. So this is very big serious problem in Fukushima. Fukushima Prefecture’s entire populations is 2 million. So about 10% are relocated to whatever places in Fukushima Prefecture.
Slide 39

Slide 39: So we are now facing a very difficult part, how to countermeasure, how to work together with them. Today I skip plant workers, emergency responder, we only concentrate on residents who were evacuated but still staying in Fukushima. They receive chronic low-dose and also they are everyday exposed to stress/fear for risks. Unfortunately, there are shortages of education, still communication very difficult, still information never realized as accurate sources, and also many rumors of image of negative contamination are prepared in these areas.
Slide 40
Slide 40: Fukushima disaster causes uncertain health effects, but not acute. Really something occurred in Fukushima. Exactly psychological, mental effects are already observed. Anxieties, anger, sleep disturbance, post-traumatic stress, so on. Because they are still residing existing radiation dose area. So there are no choice we must take care of those people who are suffering from this stress.
Slide 41
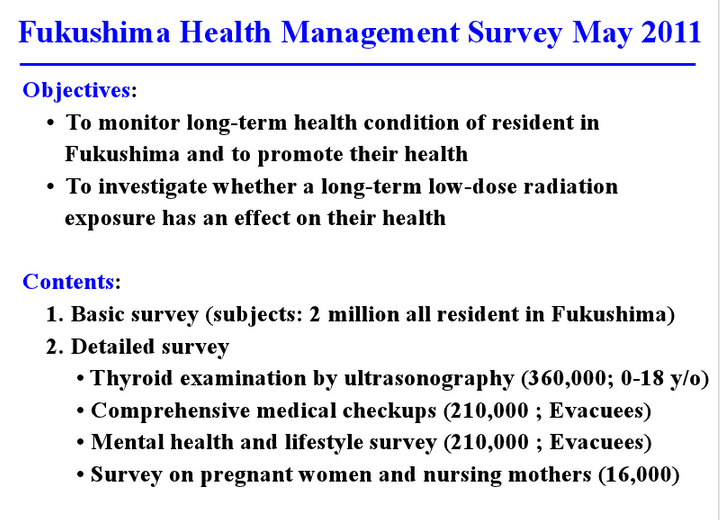
Slide 41: So we decided to start the Fukushima Health Management Survey progams. Just two months after the accident, May 2011, to set up to this type of the unprecedented health management program targeting for 2 million populations for almost whole lifespan.
Slide 42
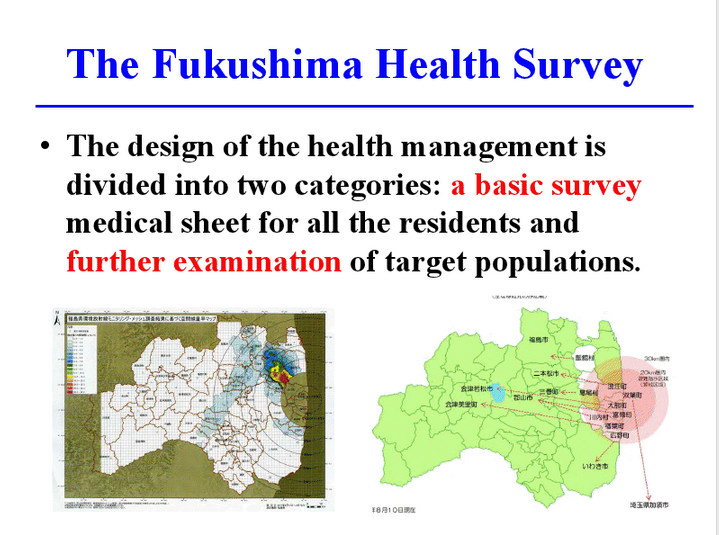
Slide 42: The design of the health management is divided to two. A basic survey is very important to evaluate the external radiation doses the first four months and then simultaneously to give or to have services on the basis of further examination of targeted population who were evacuated mainly from the contaminated areas, around 210,000 populations.
Slide 43
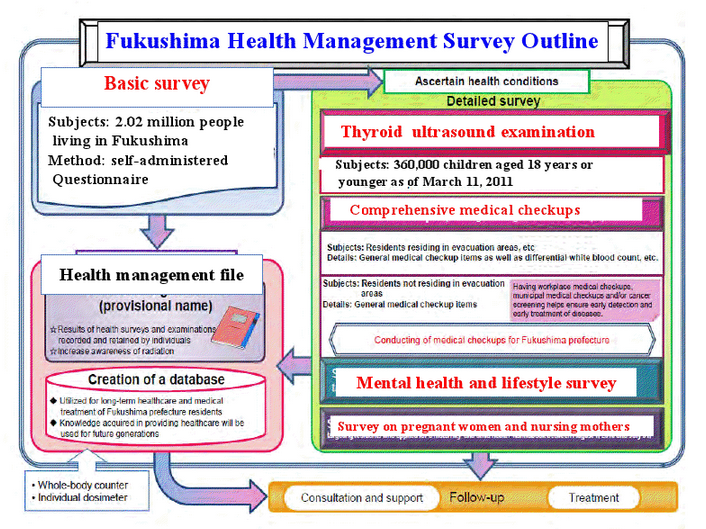
Slide 43: This slide shows outline of Fukushima Health Management Survey. This survey we are targeting 2 million population, entire population. And the detailed survey are divided four: thyroid ultrasound examination, comprehensive medical checkups, mental health and lifestyle survey, and then survey of pregnant women and nursing mother. From zero we have established this type of the survey program together with Fukushima Medical University. So therefore, our know-how from Hiroshima/Nagasaki and also from Chernobyl very much helpful for this kind of the organizations and starting of the program.
Slide 44
Slide 44: Aim is very clear. The people suffer, have anxiety and anger, have to calm down. We need to monitor for long-term health condition. This is the message to local residents. And then simultaneously we must scientifically and epidemiologically clarify to the low-dose long-term radiation effect on the human health.
Slide 45
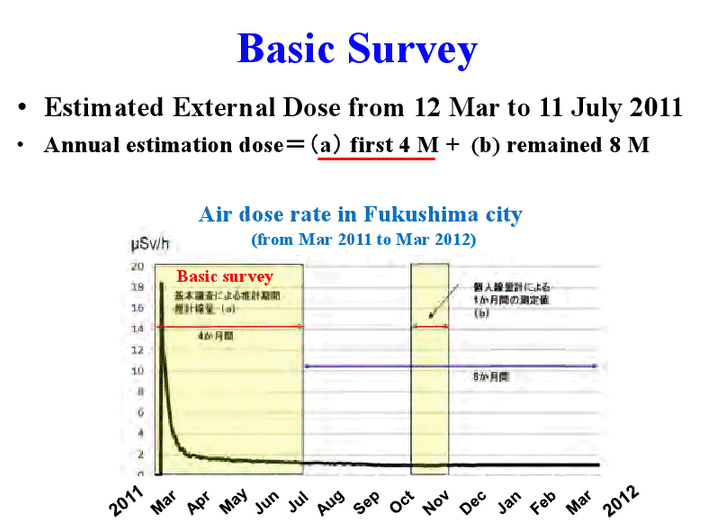
Slide 45: Basic survey means collect the record of the memory by the questionnaire and then analyze to the specialized airborne, environmental radiation doses together with the such kind of the questionnaire. Very complicated.
Slide 46
Slide 46: From March 11 to July 11, we have there on the how to move, such kind of the daily movement recorded from responding to this kind of the questionnaires.
Slide 47
Slide 47: And simultaneously time-course of airborne dose map analyzed, especially developed by NIRS, and then such kinds of the data gave us formal external radiation doses.
Slide 48
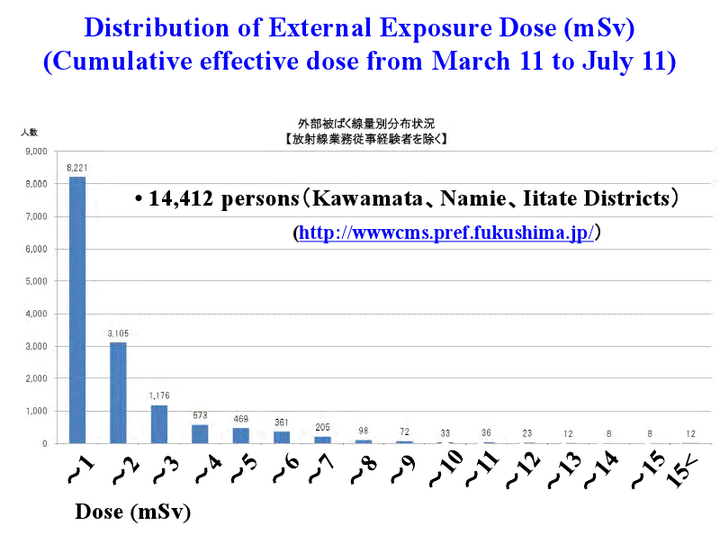
Slide 48: Very importantly, the distribution of external radiation exposure are already reported for the first four months targeting about 14,000 persons who are relatively highly exposed areas, Kawamata, Namie, Iitate districts. Almost all are less than 10 mSv, and many people are less than 3 mSv for first four months.
Slide 49
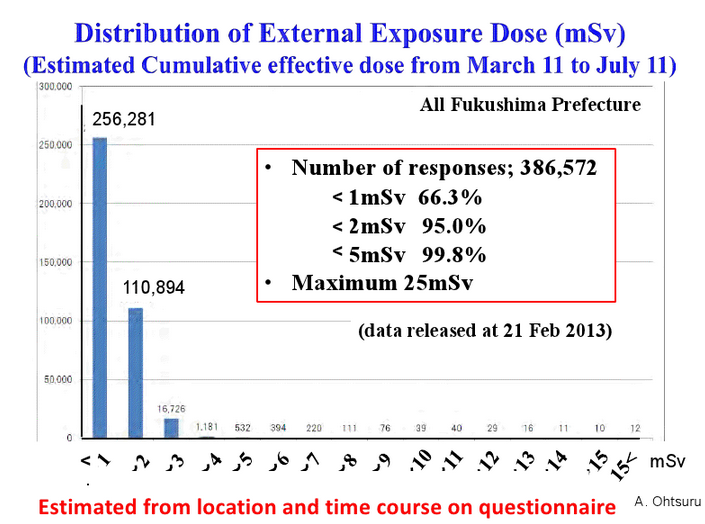
Slide 49: Recently we are reported more than 386,000 operations datas. According to these datas, estimated to local time-course of the questionnaire, external exposure dose is less than 1 mSv, 2 mSv, almost all are 5 mSv. This is a very good news for the Fukushima local residents. Fukushima now exists very low doses compared to the Hiroshima/Nagasaki and Chernobyl.
Slide 50
Slide 50: So it’s very difficult in future to confirm any increase of radiation-induced cancer through stochastic effect. However, we must continue this kind of the monitoring and also health management program.
Slide 51
Slide 52

Slides 51−52: Secondly, we are focusing on different target operations, childrens and women and other. Now I would like shortly introduce risk of radioactive iodine on thyroid in Fukushima. We are now decided age less than 18 years old, about 360,000, all children will be examined by thyroid ultrasound screening. Because of a strong pressure from the mother, the local government, and also central government. We are now started very much sophisticated first screening using the ultrasound, and then if abnormality found, second screening. Age from 0 to 18 years old. It’s the first time, except Chernobyl, we are now doing this kind of this studies.
Slide53−58
Yamashita went through these slides of thyroid ultrasound images as he kept talking. What he said in that time period is transcibed below, and each slide is accompanied by an applicable clause, in correct English, from Yamashita’s statement if any.
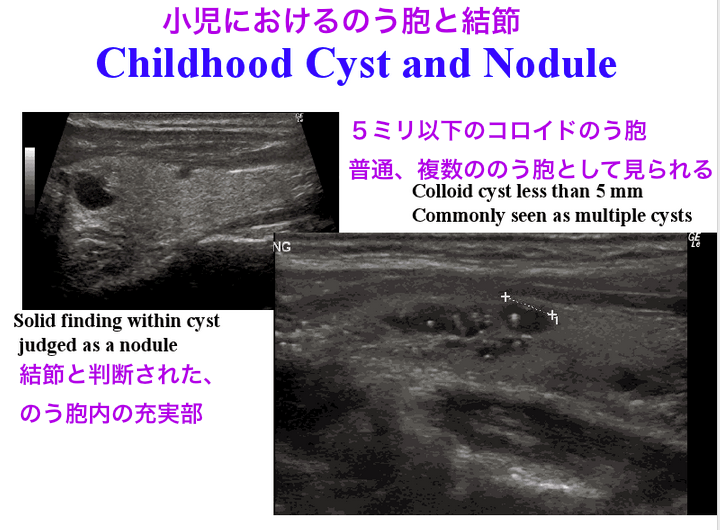
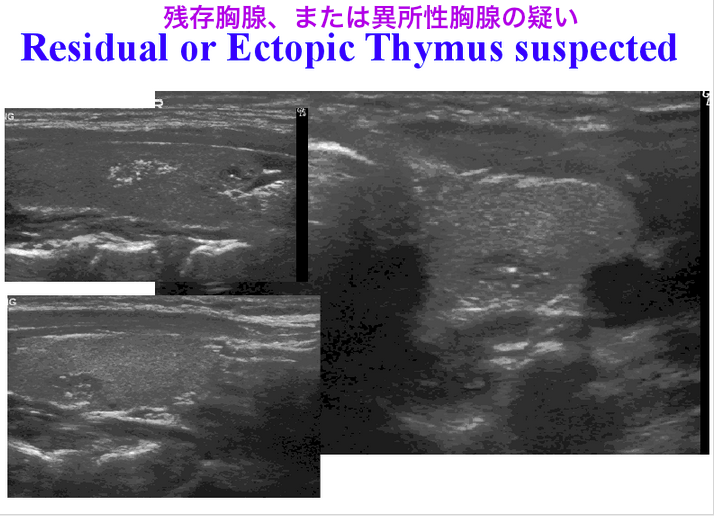
Slides 53-58: And then to find many abnormality in normal children, such as cyst, nodules, or even we can clarify ectopic or residual thymus in children within the thyroid gland. That kind of the finding are easily misdiagnosed as thyroid cancer. So therefore this is very important to clarify or make the guideline of this kind of the childhood thyroid gland using the ultrasound.
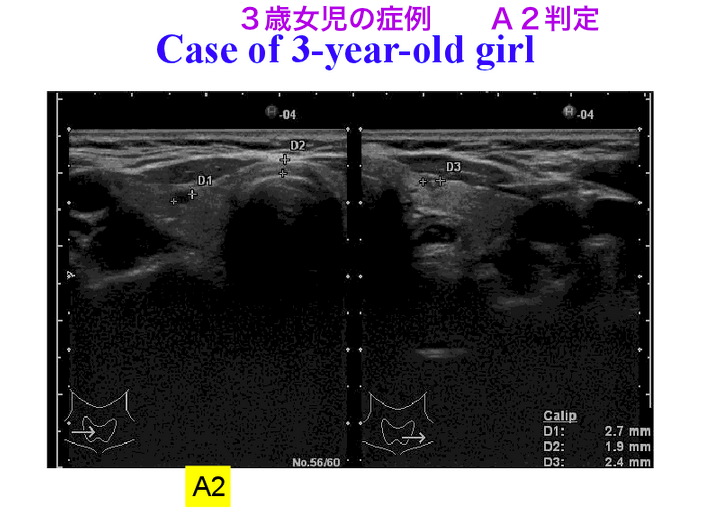
Also many cysts also discovered in children. Such kind of the small cysts, colloid clot, also discover, even 3 years old girl shows this kind of the small cysts. This is natural, spontaneously changing findings of the childrens. However, mothers very much worry in Fukushima such kind of the finding is discovered it may be due to radiation exposed by Fukushima. But before that we have never screened this kind of the thyroid for the entire childrens.
Slide 53 Many cysts and colloid clots were discovered in children.
Slide 54
Residual or ectopic thymus might be visualized by ultrasound, which might be easily misdiagnosed as thyroid cancer.
Slide 55 Many cysts and colloid clots were discovered in children.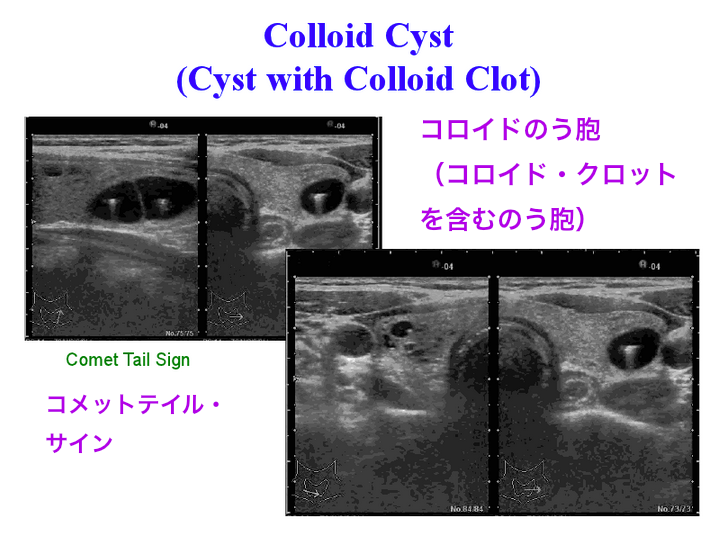
Slide 56 Many cysts and colloid clots were discovered in children.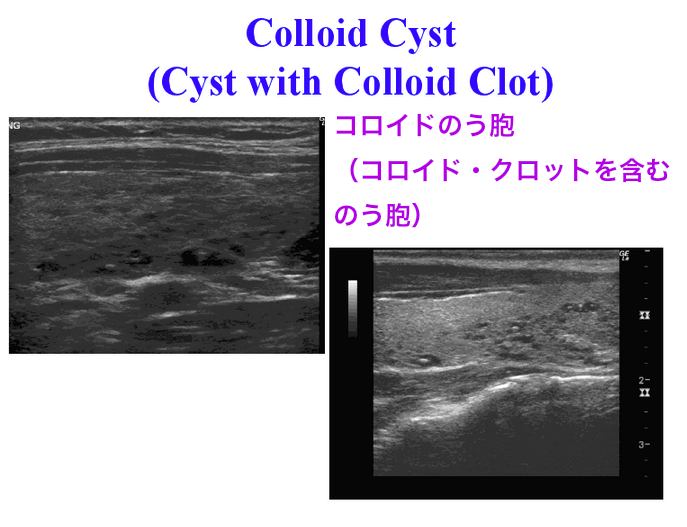
Slide 57 A 3-year-old girl with an A2 assessment (small cysts). These are natural findings in children which would change spontaneously. However, when such findings are discovered in Fukushima, mothers worry a lot whether they were caused by radiation exposure from the Fukushima accident.
Slide 58 Childhood thyroid cancer and thymus. (Yamashita did not explain this slide in particular).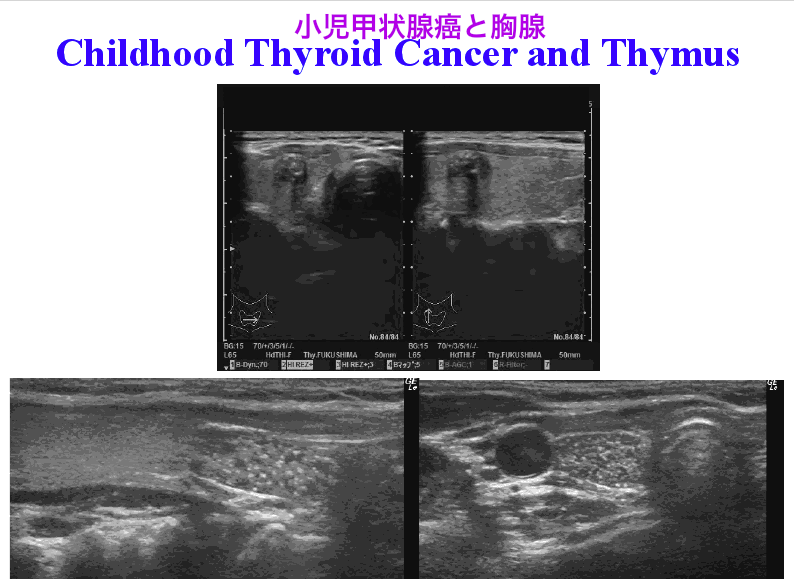
Slide 59
Slide 59: This is the recent result of thyroid ultrasound survey. We are categorized A means normal, but A completely normal not specific finding we divide it A1. Small cysts or nodules also we say A2. B, the nodules more than 5 mm or cysts more than 20 mm may introduce to the recommendation of second screening. According to the 133,000 children screening datas, we have found 99.5% the normal, but 0.5% of the abnormal, 3 clarified by second screening. This is the first data. So but this is very important to realize what is this number.
Slide 60
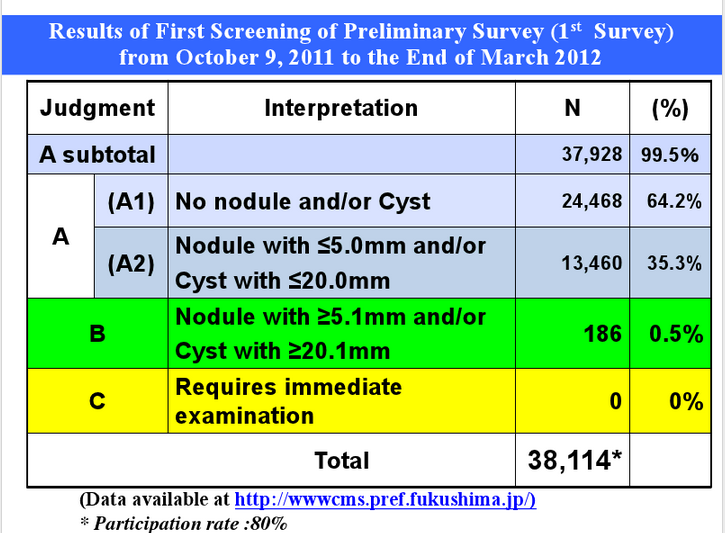
Slide 60: The first-year screening from October 2011 to the end of the March 2012, they completed about 38,000 childrens second screening. According to these data, nobody realized less than one year since after the accident, they are not related to the Fukushima accident. But the people in public concern very much this kind of the diagnosis of B, even A2, are related to the effect of radiation exposure.
Slide 61
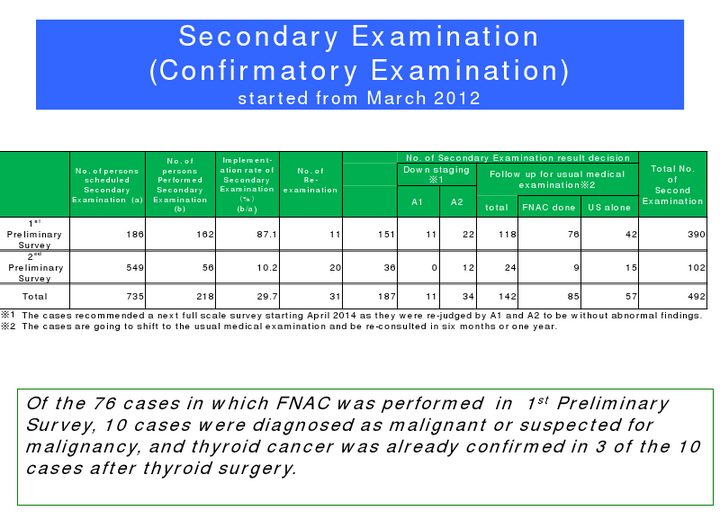
Slide 61: Results of the second examination showed, this second examination means fine-needle aspiration biopsy applied to some part of the thyroid nodule. Among them we have already operated 3 cases of childhood thyroid cancer, and 7 cases of malignancy are suspected in these area.
Slide 62
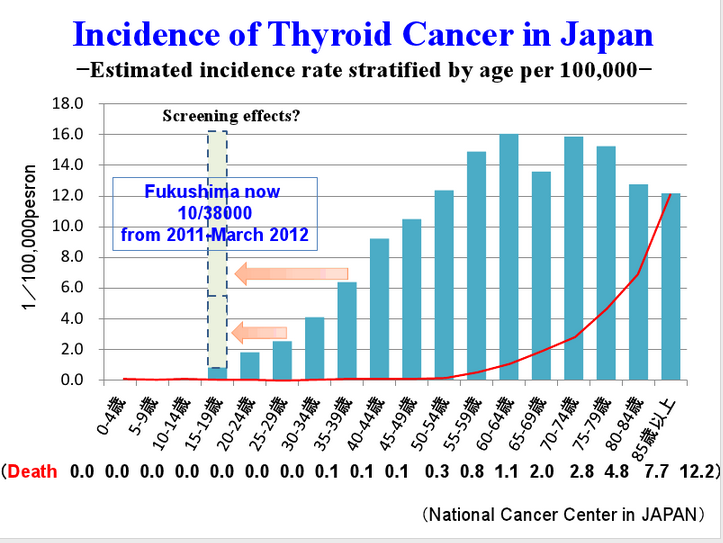
Slide 62: According to these data, everybody was surprised because this is Japanese thyroid cancer incidence, each 5 years, each 5 years are shown in blue bar. This is a cancer death rate. (showing the bottom insert) Incidence of thyroid cancer is very rare in childrens. Of course, this is true. But we started the screening in this less than 18 years old. Very much high increase of the thyroid cancers, even asymptomatic children. We are facing very much difficulties not to radiation but also this kind of the medical examination.
Slide 63
Slide 63: Now the bad news. We have a sensational news. “Over a third of Fukushima children at risk of developing cancer.” “Fukushima kids have skyrocketing number of
thyroid abnormalities.” We are being attacked by them. But this type of the mass screening activities in Fukushima led to an increase in the incidence of thyroid nodules/cysts, even cancers due to early detection of non-symptomatic cases. It is not be possible to compare the future observed thyroid cancer incidence with figures of any previous report, as the baseline risk changes due to the screening activity. We need explain carefully many times to the operations.
Slide 64
Slide 64: I also just introduced the small result of what we have done health checkups. Among 210,000, 70,000 children and adult examined, and very unfortunately, obesity and hyperlipidemia conditions increased in these evacuated people because of shortage of exercise.
Slide 65
Slide 65: And that also mental health care and lifestyle survey indicated that children and adults such kind of stress. For example, in children school performance changes, irritations, anxiety, depression, and still sensitive to earthquake and radiations. In adults, there are many cases of sleep disturbances, depression, fear of futures, agitation, discount of evacuation life. It’s a really acute phase reaction. We don’t know how long they continue. How we can intervent or care all those people.
Slide 66
Slide 66: And even pregnant women are very much concerned. But very fortunately, in Japan, there are neither any increase of miscarriage nor artificial abortions. It’s very good news. There is no obvious increased prevalence rate of congenital malformations. So we need to announce and also explain such kind of the datas.
Slide 67
Slide 67: So therefore, in Fukushima Medical University opened out to the English website Fukushima Radiation and Health, and then communicating not only to the public also into the world experts or world societies.
Slide 68
Slide 68: Finally, what we learn from Fukushima. Too early to conclude anything, but we have discussing a lot after Fukushima. First, emergency planning zone and protective action guideline should be changed. And potassium iodine (KI) policy, today I skipped, are now discussing a lot. And thirdly, most difficult part, how to communicate to the public and how to protect the public from radiation and radiation phobia. Finally, reentry and recovery policy still lacking, even we are following ICRP 101. However, in the Fukushima, it’s very difficult to communicate to the public. I really wish to cooperate with NCRP and international organizations targeting on the research/education for risk analysis, risk communication, risk management, and so on.
Slide 69
Slide 69: Once again, I would like to say thank you very much for your support to the Fukushima, and also it’s a very much honor to give a such kind of the special lecture to all of you. Thank you very much.
*****
NCRP President Boice: Yes, I certainly would like to thank Dr. Yamashita for one of the most informative and excellent presentations I’ve ever heard both on summarizing the Chernobyl experience with regard to thyroid and then bringing us up to literally to date on what’s happening around Fukushima. I mean, this is up to the minute information.