
By Yury Bandazhevsky
Revised English translation by Yuri Hiranuma
Original full version “Radioactive Caesium and Heart”https://docs.google.com/file/d/0B3fFCVXEJlbvQkluX2tocjVZd2c/edit
Thus, it is possible to make a conclusion about harmful influences of this radionuclide on the cardiovascular system after analyzing the following data: results of ECG examination of the children of various ages with varying degrees of incorporation of radioactive cesium in the body; microscopic studies of organs of individuals in the territories affected by the Chernobyl accident; and lastly laboratory experiments with animals. This effect is manifested not only due to its direct impact on cellular structures but also its indirect influences through a series of systems, in particular the nervous and endocrine systems.
A direct effect of radioactive cesium on the heart is due to its selective accumulation in the myocardial cells compared to other organs and tissues (Fig. 9 &10). Perhaps it is due to the intensive functioning of the Na+/K+ pump: since Cs-137 is similar to potassium, it is absorbed by cardiomyocytes fairly easily. This process involves the structures of cellular membranes, and this radionuclide interacts with them easily.15 This is accompanied by suppression of a very essential enzyme such as creatine phosphokinase, which is involved in the cellular energetic metabolism: accumulation, transport, and utilization of high energy phosphates. Creatine phosphokinase (CPK) catalyzes the reversible phosphorylation reaction which involves transfer of a phosphate group from adenosine triphosphate (ATP) to creatine and from phosphocreatine to adenosine diphosphate (ADP). 1
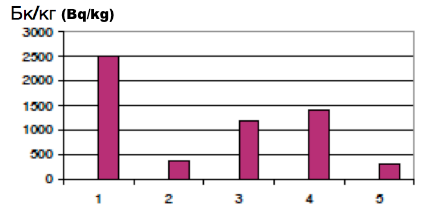
Figure 9. Accumulation of Cs-137 in organs and bodies of experimental animals
1-heart, 2-liver, 3-spleen, 4-kidneys, 5-whole body
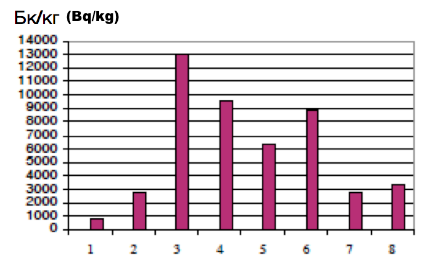
Figure 10. Accumulation of Cs-137 in the internal organs of albino rats with a daily intake of 180 Bq
1-whole body, 2-liver, 3-kidneys, 4-myocardium, 5-spleen, 6-skeletal muscles, 7-testicles, 8-lungs
Creatine phosphokinase is localized in different subcellular structures: cytoplasm, mitochondria, microsomes, nuclei, sarcoplasmic reticulum and myofibrils. According to the existing concept, mitochondrial creatine phosphokinase catalyzes the formation of phosphocreatine from ATP, which is produced within the mitochondrial matrix as a result of oxidative phosphorylation. The resulting phosphocreatine moves into the cytoplasm according to the concentration gradient or by rapid diffusion to specific isoenzymes of creatine phosphokinase and in particular to be:
· related to the structures responsible for muscle contraction; the M-line of myofibrils.
· associated with the sarcoplasmic reticulum Ca2+ adenosine triphosphatase.
· associated with postsynaptic membrane, rich in acetylcholine receptors and ATPases.
Mitochondrial creatine phosphokinase holds together the outer and inner surfaces of the mitochondrial membrane, creating its structure.1
Localization of creatine phosphokinase in the area of M-line creates conditions that allow continuous renewal of ATP to ensure proper contractile function of myofibrils (Fig. 11). The resulting creatine returns to mitochondria in order to again become a substrate for phosphorylation.
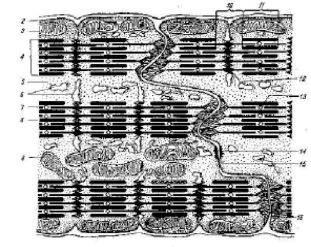
Figure 11. Intercalated disks of cardiac muscles (scheme).
1-basement membrane of cardiomyocyte, 2-sarcolemma of cardiomyocyte, 3-mitochondrion, 4-myofibrils, 5-sarcoplasma, 6-cytoplasmic network, 7-thin filament (actin), 8-thick filament (myosin), 9-intercalated disk, 10-light disk (I-band), 11-dark disk (A-band), 12-Z disk, 13-M-disk, 14-desmosome (macular adherans), 15 nexus (gap junction), 16-fascia adherens (by Bargmann & Schulce; modified).
Thus a decrease in the enzyme activity indicates serious structural and metabolic defects in the energetic complex of cardiomyocytes. This is observed as changes in the mitochondrial system in the form of an increase in the number and size of mitochondria and the increase in the number of lamellar cristae and their subsequent destruction. It is also observed as aggregation of mitochondria and changes in the number of intermitochondrial contacts (Fig.12).
 Figure
12. Aggregation, increase in the number, and increase in the size of
mitochondria of cardiomyocytes of rats with incorporation of radioactive
cesium in the body at 45 Bq/kg. Magnification X30,000.
Figure
12. Aggregation, increase in the number, and increase in the size of
mitochondria of cardiomyocytes of rats with incorporation of radioactive
cesium in the body at 45 Bq/kg. Magnification X30,000.Inhibition of the energy complex could be related to a direct influence of radioactive cesium on the membrane structure as well as an influence of several metabolites, particularly thyroid hormones, considering that these hormones have toxic effects on the mitochondrial system. 13 In this regard, activities of creatine phosphokinase are inhibited in Graves’ disease or in experimentally induced hyperhyroidism. 1 It is possible that under the influence of radioactive cesium an increased amount of free thyroxin damages myocardial cells by affecting these enzymes. This hypothesis is proven by the increase in the frequency of ECG changes that parallels the free thyroxine level in blood of children with radioactive cesium incorporation of higher than 37 Bq/kg (Fig. 13). Thus it is possible to assume the role of thyroxin in occurrence of arrhythmias.
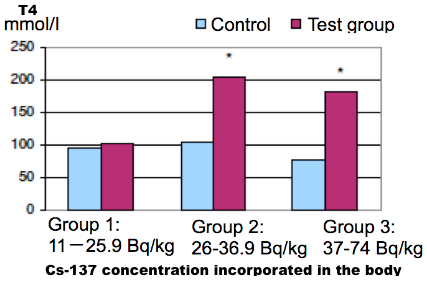
Figure 13. Dependence of serum thyroxine (T4) level in children on the amount of incorporated Cs-137 (P <0.001 between Groups 1 and 3).
In men, activity of creatine phosphokinase is greater than in women. 1 It cannot be ruled out that the vulnerability of this enzyme in myocardial cells under the influence of radioactive cesium is the leading cause of sudden deaths in men.8,29,41
It should be noted that a decrease in the activity of alkaline phosphatase in the myocardial structures is indicative of the development of degenerative processes specific for exposure to ionizing radiation. 36
The nature of structural changes, in the myocardial cells of laboratory animals with the incorporation of radioactive cesium and individuals living in areas contaminated with radioactive cesium, indicates impairment of permeability of sarcoplasmic reticulum membrane for Ca2+. This may be due to the direct effect of this radionuclide on the cell membrane as well as the radioactive rays emitted as it decays. The resulting peroxidation of fatty acid chains of phospholipids leads to changes in the cell membrane’s structure and permeability to different ions, including Ca2+ . At the same time, it naturally changes the activity of membrane-bound enzymes. Excess production of free hydroxy radicals and amplification of lipid peroxidation contribute to the destruction of cell membranes.
The Ca2+ transport system of the myocardial sarcoplasmic reticulum is actively involved in the process of contraction-relaxation of myofibrils by way of releasing and accumulation of Ca2+. If the system is damaged due to various agents, including radioactive cesium, the level of free Ca2+ in cardiomyocytes increases and the relaxation of myofibrils is disrupted.
Changes in the contractile apparatus are reflected in changes observed in the double ray refraction of myofibrils: appearance of segmental and subsegmental contractures, intracellular myocytolysis, primary cluster disintegration of myofibrils, cytolysis, and eventually coagulative or colliquative necrosis. 32
Contractive alterations of segmental and subsegmental types are defined in the polarized light by enhancement of the anisotropy of the A-band of myofibrils. They look like a radiant cross strip with cross sections of striated myofibrils between them. When examined under the light microscope, they are visible due to the greater density and eosinophilia. Ten days’ worth of radioactive cesium incorporation by rats of Vistar line (cesium concentration was 60-100 Bq/kg) also led to these alterations (Fig. 14).
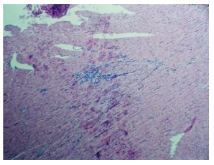
Figure 14. Histological section of animal myocardium after incorporation of radioactive cesium in food (concentration in the body at 100 Bq/kg). Diffuse contracture in myofibrils of cardiomyocytes. Diffuse myocytolysis. Focal infiltration of lymphohistiocytic cells. Stained with hemotoxylin and eosin. Magnification X125.
In the primary cluster disintegration of myofibrils, the isotropic spaces are found between anisotropic clusters (Fig 15). This, unlike contractures, is severe and irreversible damages to cardiomyocytes indicating their death. It should be noted that primary cluster disintegration is often found in acute cardiac insufficiency. 30,31
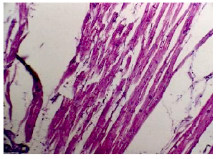
Figure 15. Histological section of myocardium of a woman who died in childbirth. Radioactive cesium concentration in heart at 105 Bq/kg. Primary cluster disintegration of myofibrils. Loosening of muscle fibers. Intermuscular edema. Stained with hematoxylin and eosin. Magnification X250.
Cytolysis or in vivo autolysis of myocardiocytes is also an irreversible condition. It tends to be diffuse under the influence of radioactive cesium (Fig. 16,17).
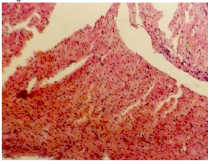
Figure 16. Histological section of animal myocardium after incorporation of radioactive cesium (concentration in the body at 900 Bq/kg). Diffuse myocytolysis. Pronounced intertissue edema. Stained with hematoxylin and eosin. Magnification X125.
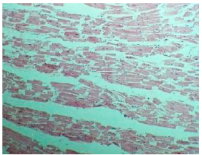
Figure 17. Histological section of myocardium of a 43-year-old Dobrush resident who died suddenly. Raioactive cesium concentration 45 Bq/kg. Diffuse myocytolysis. Intermuscular edema. Fragmentation of muscle fibers. Stained with hematoxylin and eosin. Magnification x125.
The above changes are observed not only under the exposure to radioactive cesium but also when there are metabolic damages due to intoxication, hypoxia, or functional overload 14,24,40 and under the influence of extreme environmental factors contributing to the development of stress reactions. 27,28,31 It is observed that these reactions occur when the Ca2+ concentration in cardiomyocytes is increased. 28
The leading role in the mechanism of injury is played by the effects of catecholamines (noradrenaline, adrenaline) on the beta-adrenergic receptors of the myocardium. This does not have any connection with ischemic damage to the heart. 28
The total scheme of the effects on heart is influenced by a wide variety of factors through stress reactions. High concentrations of catecholamines increase the number and timing of opening of the voltage-dependent and receptor-dependent calcium channels, resulting in the accumulation of Ca2+ in cardiomyocytes. In addition, cells of conducting system are damaged earlier and to a greater degree, since they have low resting potential and the input ion current, which is responsible for the action potential, is primarily calcium.10 Moreover, this system has predominantly adrenergic innervation. 28
As a result of the process, cells end up with a high concentration of Ca2+. When these Ca2+ are inappropriately released from the cell, arrhythmias, or rhythm disturbances can occur. We emphasize that it is directly related to the function of the cationic pumps. A significant role in the energy supply for the pump is played by the creatine phosphokinase and glycolytic systems. 28 In order to cause relaxation of myocardium and break bridges between thin actin and thick myosin myofibrils, it is necessary to coordinate both of these systems. This includes sarcoplasmic reticulum ATPase, which transports Ca2+ back into the cistern of sarcoplasmic reticulum. It should be noted that this is an energy-requiring process, comprising nearly 15% of all energetic consumption of the cardiac muscles. 25
Considering the duration of influence of radioactive cesium on people living in the contaminated territories and the suppression of noradrenaline production in the cells of cerebral hemispheres, 23 it is not hard to imagine the leading role of catecholamines in causing contractures of muscle fibers. It could just happen in cases of strong stress reactions. In reality, accumulation of Ca2+ in the cells under the influence of radioactive cesium can occur due to the energy deficit caused by damage to the energy supply system within the cell membranes, including mitochondria and structures of sarcoplasmic reticulum. That is why the cells cannot release Ca2+ in a timely manner. Calcium ions enter the cells very intensively due to the destruction of membrane phospholipids by free radical hydroxyl groups. In this situation it does not take much effort to cause significant myocardial damage. Death of cardiomyocytes can occur due to prolonged energy deficits, caused by physical exertion, acute infectious processes and alcohol intoxication.
Cardiac activity could be stopped by increasing the concentration of radioactive cesium in the body. In particular, a rapid administration of a large amount of the Cs-137 radionuclide, reaching the concentration of 1,000 Bq/kg within 5 days, caused cardiac arrest in rats. In this case the radioactive agent itself became the direct cause of death. To a lesser degree, the source of recontractions of myofibrils of cardiomyocytes in the presence of radioactive cesium accumulation could be an emotional stress, resulting in the release of catecholamines. This is due to the fact that in long-term cesium toxicity, there is a progressive suppression of function of the sympathetic nervous system, reducing the adaptive reserve of the body.17 At the same time it is impossible to exclude the role of catecholamines in cardiac damage under the influence of radioactive cesium.
This has been confirmed by the results of clinical and laboratory testing of children with chronic gastrointestinal pathology. There was a directly proportional relationship between the frequency of hypersympatheticotonic variant of the autonomic nervous system reactivity and the amount of radioactive cesium in the body. Based on the above data, it is necessary to conclude that the energy deficit in the calcium transport system, appearing during the radioactive cesium incorporation, leads to disruption of cardiac rhythm, disorders of contractile apparatus of cardiomyocytes, and eventually cardiac arrest.
Injuries to the cardiovascular system could not be examined separately from other organs and systems, particularly the kidneys. As the main organ of excretion of radioactive cesium from the body,16 kidneys are significantly affected even at a small Cs-137 concentration. Kidneys also undergo similar damaging effects as the cardiovascular system, first and foremost in the glomerular apparatus. 6,7 In the muscle fibers within the arterioles, there are changes identical to those observed in the myocardium. Contractures of myofibrils lead to a prolonged spasm of the arterioles, stopping the circulation in the structures of the nephron. Deaths of cellular elements form a specific structural change in the glomeruli, a phenomenon called melting icicles. Dystrophic and necrobiotic changes gradually appear, accompanied by wrinkling and fragmentation of the glomeruli (Fig. 18 &19).
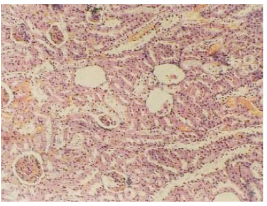
Figure 18. Histological section of albino rat kidney with a radioactive cesium concentration in the whole body at 900 Bq/kg. Necrosis and fragmentation of glomeruli with cavity formation. Necrosis and hyaline droplet dystrophy of tubular epithelium. Stained with hematoxylin and eosin. Manification x250.
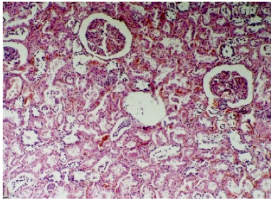
Figure 19. Histological section of kidney of a 71-year-old female patient in Gomel. She died of adhesions of abdominal cavity and right lung acute lobar pneumonia with consolidation and fibrino-purulent component, complicated by bilateral pulmonary edema. Radioactive cesium concentration in kidneys was 300 Bq/kg. Fluid accumulation in glomerular cavities. Hyaline droplets and hydropic dystrophy of tubular epithelium. Interstitial tissue edema. Stained with hematoxylin and eosin. Magnification x125.
Cavity formation without any marked cellular reaction is typical as the influence of radioactive cesium on kidney’s tissues. With the ability to cause hyper-contractions (excess contractions) of muscle fibers in arterioles, this radionuclide damages the processes of vascular microcirculation in kidneys. It should be noted that there is an absence of necessary inflammatory reactions of the body in response to the damages in kidneys and other organs. In our opinion, this is due to the suppression of synthesis of biologically active substances, such as inflammatory mediators, in specialized cells.
Damaged glomeruli cease functioning. Histologic characteristics of kidneys under the influence of radioactive cesium are the same as those of thrombotic microangiopathy. 2 This is no coincidence. In both cases, the microcirculatory channeling system of nephron is blocked at the level of arterioles, leading to necrobiotic processes.
Development of renal insufficiency is the reason for accumulation of metabolic waste products in the body. They have toxic effects, along with the toxic effects of radioactive cesium itself, on the vital organs and systems. Also characteristic are the inflammatory processes of serous membranes, particularly of pericardium (Fig. 20) and pleura (Fig. 21).
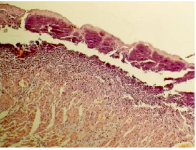
Figure 20. Histological section of animal myocardium with Cs-137 incorporation at 900 Bq/Kg in the body. Infiltration of epicardium and pericardium with neutrophils and lymphocytes. Pronounced myocytolysis. Stained with hematoxylin and eosin. Magnification x125.
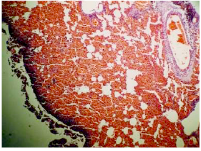
Figure 21. Histological section of animal lung with Cs-137 incorporation at 900 Bq/kg in the body. Plethora from rupture of blood vessels in the alveolar lumen. Infiltration of visceral pleura with neutrophilic leukocytes, lymphocytes and histiocytes. Stained with hematoxylin and eosin. Magnification x125.
Injuries to the vascular system of kidneys may be one of the main reasons for the increase in blood pressure, especially diastolic pressure, in children. However, considering the hidden, latent course of this pathological process, it could only manifest later, after ordinary medical treatments proved insufficient. Therefore, regular assessment of kidney and cardiac function must be done in children living in areas contaminated with radioactive cesium, using modern laboratory and technological diagnostic methods.
Liver is also negatively affected by the influence of radioactive cesium. Individuals who lived in the Gomel region had significant levels of radioactive cesium in their liver. 6 In most of those cases, histologic examinations revealed marked dystrophic and necrobiotic changes in the hepatocytes (Fig. 22).
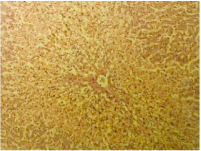
Figure 22. Histological section of liver from a 40-year-old Gomel resident who died of sudden death. Radioactive cesium concentration in the liver was 142 Bq/kg. Fat and protein degeneration with necrosis of hepatocytes. Stained with hematoxylin and eosin. Magnification x125.
Similar changes were observed in the experimental animals under the influence of radioactive cesium. Immediately there was a disruption of the hepatocyte function, particularly synthetic and detoxifying functions.
Impairment to the synthetic function of hepatocytes is manifested as a progressive decrease in the synthesis of L1-globulin and L2-globulin with an increasing concentration of radioactive cesium in the body. This will undoubtedly affect the state of metabolism in other organs, including the heart.
Oxidation of steroid hormones, especially the adrenal cortical hormones, takes place in the liver. Also destruction of catecholamines, the hormones of adrenal medulla, noradrenaline and adrenalin, takes place by way of methylation reaction. A huge role of liver is detoxification of ammonia, by utilizing it in the synthesis of urea. Inefficiency in both synthetic and detoxifying functions of liver leads to the appearance of metabolic dysfunction, which leads to an adverse effect on the state of myocardium.
Thus, metabolic dysfunction, occurring in the body incorporating radioactive cesium, may contribute to disturbances in the structure and function of cardiomyocytes.
Conclusion
While working on this book, I kept thinking about the need to inform every civilized individual of the dangers of radioactive substances when incorporated into the body. Unfortunately, the attitude of the present society to this issue is, at best, indifference. We pay a very high price for this in the form of human lives. Intelligent ignorance leads to a tragedy. To a great extent the blame rests on medical scientists. Not only did they not try to inform population using previously obtained data, but they did not study adverse changes in the body due to incorporation of radionuclides.
I am aware that this little book cannot make up for the lack of information on the existing problem. Nevertheless, I hope it will raise some interest, leading to discussion of the problem. This will undoubtedly be helpful.
Based on the information presented, some conclusions can be drawn.
Whether we like it or not, radionuclides, especially radioactive cesium, are present in our environment. Without any protective measures, they enter a human body mainly through food and water, becoming incorporated in organs and tissues. The greatest danger to human life represents the incorporation of radioactive cesium in the cardiac muscles of growing bodies.
When myocardial cells are penetrated by the radionuclide Cs-137, structural and metabolic changes follow, leading to the energy deficits and disruption of their main functions, and in some cases death. A series of changes occur, indicating direct damage of the cardiac muscles as well as damage to many organs and systems regulating its activity. Cardiomyocytes are damaged not only directly due to radioactive cesium but also due to natural metabolites when there is disruption in their production, transport, binding, excretion, and degradation (Fig. 23).
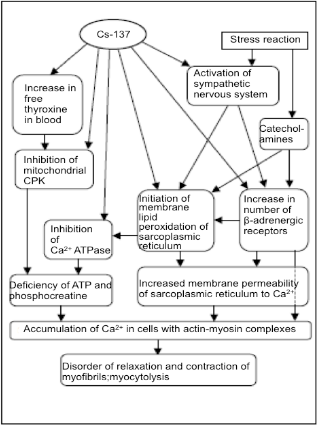
Figure 23. Diagram for the influence of radioactive cesium on cardiomyocytes
(CPK=creatine phosphokinase, ATP=adenosine triphosphate)
Degree of severity of pathological changes is directly dependent on the amount of radioactive cesium in the body and cardiac muscles. Long-term incorporation of the radionuclide in the body greater than 30 Bq/kg is highly undesirable, possibly leading to serious consequences.
In most cases the effect of existing concentration of radioactive cesium in the body (10-20 Bq/kg) does not lead to death. However, the influence of radioactive cesium on the energy apparatus of cardiomyocytes significantly reduces their adaptive capacity. It might become impossible to function in a variety of stressful and ordinary situations, such as physical and mental stress, hypoxia, extreme temperature fluctuations, drinking alcohol, infections, and allergic diseases.
It should be recognized that radioactive cesium is a potent damaging agent and it should be treated as a delayed poison to cell actions.
Undermining the energetic mechanism for cardiomyocytes, it causes cardiomyopathy, characterized by cardiac rhythm disturbances, abnormalities in myocardial contractility, and spasms of peripheral blood vessels. It should be noted that the effect of incorporated radioactive cesium on humans and animals suggests its involvement in energetic and metabolic processes, primarily as a chemical element rather than a source of radiation. Nevertheless, the latter involvement, as a source of radiation, cannot be excluded completely. This is especially pronounced with prolonged exposure to small amounts of this radionuclide. The main reason for pathological changes of the kidney due to the influence of radioactive cesium is arteriole spasm, which causes necrosis of the glomerular loops and destruction of the nephron structures. The vasoconstrictive effect of cesium was noted by S.S. Botkin in 1888. 11
Therefore, radioactive cesium is one of the major etiologic factors in high blood pressure in children living in radioactively contaminated areas. This has been confirmed by numerous observations. 20
As the basis of prophylaxis of cardiovascular diseases in population living in the areas affected by the Chernobyl accident, relevant issues include the reduction of the amount of radionuclides, above all radioactive cesium, by reduction of its content in food as well as its elimination from the body with adsorbing agents. These measures will play an important role in improving the metabolism of myocardium.
Bibliography
1. Antipenko, AE, Kalinski MI, Lyzlowa SN. Myocardial Metabolic Regulation under Different Functional Conditions. Russia: University Publishing House; 1992.
2. Antonovych TT, Mostofi FK. Atlas of Kidney Biopsies. Washington, D.C.: Armed Forces Institute of Pathology; 1980.
3. Bandazhevsky GS. The state of cardiac activity in children living in areas contaminated with radionuclides. Medical aspects of radiation exposure on the population living in contaminated areas after the Chernobyl accident: proceedings of the International Scientific Symposium. Gomel; 1994.
4. Bandazhevsky GS. Functional modifications of myocardium in postnatal ontogenesis under the influence of incorporated radionuclides. PhD thesis. Moscow; 1996.
5. Bandazhevsky YuI. Pathophysiology of Incorporated Radiation. Gomel: Gomel State Medical Institute; 1997.
6. Bandazhevsky YuI. Pathology of Incorporated Radiation. Minsk: Belarusian State Technical University; 1999.
7. Bandazhevsky YuI. Medical and Biological Effects of Radiocesium Incorporated into the Human Organism. Minsk: Belrad; 2000.
8.. Bandazhevsky YuI, Bandazhevsky GS. Effect of radioactive elements, getting in the environment as a result of the Chernobyl accident, on the state of myocardium. In: Bandazhevsky YuI, Lelevich VV, et al (eds.) Clinical and Experimental Aspects of the Effect of Incorporated Radionuclides upon the Organism. Gomel: Gomel Medical Institute; 1995.
9. Bandazhevsky YuI, Matjukhina TG, Zelenko GA. Ultrastructural response of the ventricular cardiomyocytes to the radiocaesium penetration. In: Morphological and Functional Aspects of the Radiocesium Effect Upon the Processes of Antenatal and Postnatal Development. Gomel: Gomel Medical Institute; 1998. p15-20.
10. Bershova TV, Bakanov MI, Bokeria LA, et al. Cellular mechanisms of calcium regulation of cardiac rhythm in children with ectopic arrhythmias. Vopr Med Khim 1994 Jul-Aug;40(4):50-3.
11. Botkin SS. Effect of rubidium salts and cesium on heart and blood circulation. MD thesis. St. Petersburg; 1887-1888.
12. Vatutin NT, Kalinkina NV. Damaging of heart with cytostastics. Cardiology 1998;11:53-57. [sic]
13. Vecherskiy GA, Baranov LG, Lisyutin VG. Handbook of Clinical Electrocardiography. Minsk, Belarus; 1985.
14. Golancev NE, Sazontov TG. Changes in resistance of Ca-transporting system of myocardial sarcoplasmic reticulum during "urgent" and "long-term" adaptation to physical load. Biull Eksp Biol Med (Bulletin of Experimental Biology and Medicine) 1998 Jan;125(1):40-4.
15. Dolgii NL, Danilova VV, Tregubov VS. The localization of radioactive cesium in bovine muscle tissue. Radiobiologiia 1992 Mar-Apr;32(2):284-7.
16. Zhuravlev F. Toxicology of Radioactive Substances. 2nd ed. Revised. Minsk: Energoatomizdat;1990.
17.Zaitsev VA, Balakleevskaia VG, Petrenko SV. The functional status of the hypophyseal-adrenal cortical adaptation system in children in Byelarus living under the action of low doses of radiation after the accident at the Chernobyl Atomic Electric Power Station. Radiobiologiia 1992 Jul-Aug;32(4):483-7.
18. Health in Europe. The 1993/1994 Health for All Monitoring Report. WHO Regional Publications, European Series, No.56. Copenhagen; 1994.
19. Ivanov GG, Smetnev AS, Syrkin AL, et al. The basic mechanisms, principles of prediction and prevention of sudden cardiac death. Kardiologiia 1988;12: 64-73. [sic]
20. Kienja AI, Ermolitski NM. Vegetative components of the reactivity of children with different levels of incorporated 137Cs. In: Bandazhevsky YuI (ed.) Structural and Functional Effects of Radioisotopes Incorporated by the Organism. Gomel; 1997. p61-63.
21. Bandazhevsky YuI, Lelevich VV Strelkov VV, et al (eds.) Clinical and Experimental Aspects of the Effect of Incorporated Radioisotopes upon the Organism. Gomel; 1995.
22. Konoplja EF, Bagel IM, Shafranovskaja EV. Effect of low doses of ionizing radiation on the activity of the Ca2+ ATPase of sarcoplasmic reticulum of skeletal muscle. Belorussian Academy of Sciences Report (Biological Series) 1996;40(3): 86-89.
23. Lelevich VV, Doroshenko EM. Effect of incorporated radioisotopes upon the pool of neurotransmitters in rat brain. In: Bandazhevsky YuI, Lelevich VV. (eds.) Clinical and Experimental Aspects of the Effect of Incorporated Radioisotopes upon the Organism. Gomel; 1995. p74-88.
24. Malyhina AP. Bioelectrical activity of cardiomyocytes of irradiated organism during hypoxia. PhD thesis. Minsk; 1998.
25. Mann T, Goldberg S, Mudge GN Jr, Grossmann W. Factors contributing to altered left ventricular diastolic properties during angina pectoris. Circulation 1979 Jan;59(1):14-20.
26. Marey AN, Barkhudarov RM, Novikova NJ. Global Cs-137 Fallout and the Human. Moscow: Atomizdat;1974.
27. Meerson FZ. Adaptive Medicine:The Mechanisms and Protective Effects of Aaptation. Moscow: Hypoxia Medical LTD; 1993.
28. Meerson FZ. Primary stress-induced myocardial injury and cardiac arrhythmia. Part I Kardiologiia 1993;33(4):50-59. Part II Kardiologiia 1993;33(5): 58-64.
29. Miliutin AA, Kirpicheva TM, Lobanok LM. The effect of incorporated cesium-137 on the structure of the erythrocyte membranes. Radiobiologiia 1993 Mar-Apr;33(2):302-6.
30. Nepomnyashchikh LM. Basic forms of acute injury to cardiomyocytes determined by polarized microscopy of myofibrils. Biull Eksp Biol Med 1996;121(1): 4-13.
31. Nepomnyashchikh LM. Structural reorganization of the myocardium during exposure to extreme environmental conditions. Morfologiia 1997;112(6): 18-24.
32. Nepomnyashchikh LM. Morphology of adaptive myocardial reactions under extreme environmental influences. Bulletin of Russian Academy of Medical Sciences 1997;3: 49-54.
33. Nesterenko VB. Scale and Consequences of the Chernobyl Accident in Balarus, Ukraine and Russia. [sic] Minsk: Law and Economics; 1996.
34. Paukov VS, Protsenko DD. Recombination mitochondrial transformations in damaged cardiomyocytes. Biull Eksp Biol Med 1998 Mar;125(3):244-50.
35. Poliakova IA, Shornikova MV, Samorukova IV, Chentsov IuS. Cardiomyocyte chondriome ultrastructure after clinical death and in the postresuscitation period in rats. Biull Eksp Biol Med 1999 Jan;127(1):95-100.
36. Schultz-Heсtor S. Radiaton-induced heart disease: review of experimental data on dose reponse and pathogenesis. Int J Radiat Biol 1992 Feb;61(2):149-60.
37. Sidorenko GI. Prevention of cardiovascular diseases: urgent task of modern medicine. Medical News 1999; 1-2: 4-8.
38. Stepanov, YV, Voitsitskii VM, Preobrazhenskaia TD, et al. Effects of irradiation on fatty acid structure of membrane lipids of the sarcoplasmic reticulum. Radiobiologiia 1992 Nov-Dec;32(6):807-14.
39. Bandazhevsky YuI (ed.) Structural and Functional Effects of Radioisotopes Incorporated by the Organism. Gomel; 1997.
40. Khitrov NK, Paukov VS. Cardiac Adaptation to Hypoxia. Moscow: Meditsina; 1991.
41. Shevchenko AS, Gabai VL, Kobialko VO, et al. Increased plasma membrane permeability for Ca2+ in radiation-induced thymocyte apoptosis.. Radiats Biol Radioecol 1997 Mar-Apr;37(2):220-7.
No comments:
Post a Comment